Africa Obesity and Health Chat
Africa, Sub-Saharan
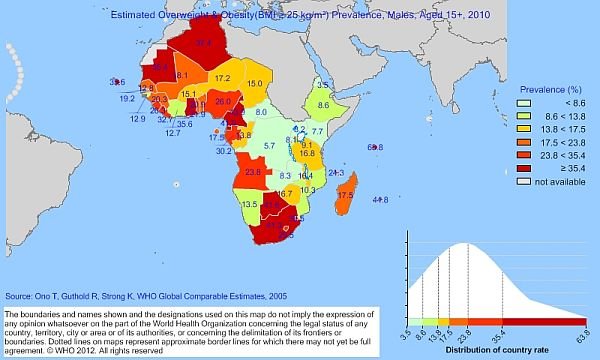
In parts of sub-Saharan Africa, there has been a tradition of some rulers being overweight or obese, a tradition that has continued through to the modern era. As well as this, the increasing affluence of some areas has led to a rise in the prevalence of obesity among the middle class, particularly westernized families.
From the late 1980s, but especially during the 1990s and the 2000s, the impact of human immunodeficiency virus (HIV) and acquired immunodeficiency syndrome (AIDS) has been devastating, and AIDS is often called “slim” in Africa because of the wasting effect it has on its victims. This has led some people to think that those who are overweight or obese are less likely to be suffering from AIDS, although this, obviously, is not the case. In former French West Africa, especially the northern region, obesity has not been a major problem until recently. A 1975 study by Dutch researchers R. De Hertogh, I. V. Vanderheyden, and M. de Gasparo of the glucose tolerance in the Toubou Broayas of northeastern Niger found that obesity was unknown in their community because of diet and physical activity.
Although obesity remains relatively rare in Mauritania, it has been found that a very significant number of patients involved in treatment for cardiology problems have been suffering from obesity. In a study conducted in 2000 by M. L. Ba of the Centre Hospitalier National, Nouakchott, Mauritania, he found that just over a third of patients involved in cardiology treatment were obese. Of the 227, 187 were women and 40 were men, illustrating a much higher level of obesity among women.
There have been a number of studies in Burkina Faso, which aimed to confirm the study by Dr. Ba in Mauritania, linking obesity to cardio-vascular problems. A study in 2001 by D. Ye, Y. J. Drabo, D. Ouedraogo, A. Samandoulougou and A. Sawadogo in Ouagadougou, the capital of Burkina Faso, showed the extremely low levels of obesity. Of the 1,470 students from primary schools and secondary schools, there were only 28 overweight cases, and only 4 of obesity-one of these four students having high blood pressure.
In Senegal, with a much higher urban population, there is an increased prevalence of obesity. These people have been shown to have a much greater likelihood of having problems from heart disease and asthma. In Guinea, a study by N. M. Balde, et al. of the Endocrinology Service, into tuberculosis and diabetes in Conakry, the capital of the country, the condition was closely associated with obesity. The much higher levels of the urban population in the Côte d’Ivoire, and the affluence of the population in Abidjan, the capital, has seen an increase in obesity in recent years among the urban middle class, as has also happened in Lome, the capital of Togo, and Cotonou, the capital of Benin.
In the former British colonies of West Africa, obesity has also been a problem in some areas. In Gambia, where there has been much tourism and increased urbanization, a study in 2006 by M. Siervo, et al. of the MRC Human Nutrition Research, Elsie Widdowson Laboratory, Cambridge, United Kingdom, has shown the Gambian population to be far more accepting of obesity, perhaps influenced by the increasing levels of obesity in their society, than Americans. A 1998 study in Sierra Leone has shown that the Mende tribe-which makes up nearly a third of the country’s population, has an increased prevalence of obesity-the war and widespread food shortages in Sierra Leone resulting in a decline in obesity levels in recent years, even though the recent civil war has ended.
There have been a number of studies of obesity in Ghana; that in 2005 by F. Ofei of the Endocrine and Metabolic Clinic, Department of Medicine and Therapeutics, University of Ghana Medical School, Accra, published in the Ghana Medical Journal, is significant.He highlighted obesity as a major and preventable condition. Dr. Ofei outlined a range of strategies largely around increased education of the population, as many people, through greater affluence, went through “an economic and nutrition transition.”
Nigeria, traditionally the wealthiest country in West Africa-and the one with the largest and richest urban elite-continues to have a major problem with obesity. As with all countries, it is difficult to survey the general public, so E. N. Obikili and L. O. Nwoye of the Department of Anatomy, College of Medicine University of Nigeria, Enugu Campus, conducted a survey of a cross-sectional study of students at the University of Nigeria Enugu Campus. Rather than collecting data, they were aiming to work out an accurate method of figuring out levels of obesity in the country, and concluded that the body mass index (W/H2) was the most suitable index to employ. However, the level of obesity, however measured, has certainly been particularly dramatic among some women.
A study by N. P. Edomwonyi and P. E. Osaigbovo of the Department of Anaesthesia, University of Benin Teaching Hospital, Benin City, Edo State, into women scheduled for cesarean section, showed that 50.7 percent were obese. In Liberia, owing to the poverty of the country and the incessant civil strife since 1979, the level of food available has been low, and consequently, the country has not faced a major problem of obesity. Similarly, in Guinea-Bissau, Cape Verde Islands, and São Tomé e Principe, all former Portuguese colonies, there has not been a problem of obesity; neither has there been a problem in the former Spanish colony of what is now Equatorial Guinea.
In former French Central Africa, there are areas of recent affluence, and this reveals itself in the increasing problems of obesity in Cameroon, Gabon, and Congo. A study in 2007 in Cameroon, by researchers from the Department of Community Health and Psychiatry, University of the West Indies, Mona Campus, Kingston, Jamaica, has shown that 36.3 percent of urban men are overweight, with 47.1 percent of women from urban areas-compared with 9.5 percent of women and fewer men from rural parts of the country.
The seriousness of the problem in the region is shown in a study for Gabon, of the 108 patients suffering from diabetes who sought treatment at the Internal Medicine Department of the Libreville Hospital Center, 64 of them were suffering from being overweight or obese. In the remainder of former French Central Africa, food shortages has resulted in malnutrition in some parts of Chad and to a lesser extent the Central African Republic, with obesity not being a problem. This was also the case in the Sudan, Ethiopia, and Somalia, as well as Djibouti. However, the 19th-century explorer Sir Samuel Baker in he Albert N’Yanza: Great Basin of the Nile (1866) refers to a custom by which wives of the King of Kisoona were forced to consume large quantities of milk-up to a gallon daily-thereby becoming obese, or face a whipping. It is a custom that has long fallen out of practice.
In East Africa, in Uganda, there has not been a major problem with obesity, although Idi Amin, who ruled the country from 1971 until he was overthrown in 1979, became noticeably overweight. In Kenya, the prosperity in the country and the much larger middle class has seen a steady increase in obesity and its related problems such as diabetes. The affluence in parts of neighboring Tanzania has resulted in obesity there. As a result, there have been a number of studies; the most detailed probably being that by C. N. Nyaruhucha, et al. of the Department of Food Science and Technology, Sokoine University of Agriculture, Morogoro, into the level of obesity of students of different ages in schools and other educational institutions in the city of Morogoro, in the southern highlands of Tanzania, west of Dar-es-Salaam. It shows that as much as 70 percent of younger children were not aware of the medical problems with obesity, and married adults had an obesity rate of 22.2 percent compared to 4.7 percent for unmarried adults.
The Democratic Republic of the Congo, formerly Zaire, there have been a level of obesity in the govern Africa, Sub-Saharanment circles with Mobutu Sese Seko (1930–97), president from 1965 until 1997 was slim when he came to power but became steadily overweight during his long period of rule, and Laurent Kabila (1939–2001), who seized power from him in 1997 being significantly overweight. Jonas Savimbi (1934–2002), the leader of the rebel UNITA movement in Angola was also overweight in his latter years.
In former British southern Africa, the affluence of much of the region and larger urban areas has led to greater levels of obesity, with the Zimbabwean nationalist leader Joshua Nkomo (1917–99) being the most well-known African leader to suffer from obesity, as did King Sobhuza II of Swaziland who reigned from 1899 until 1982. President Paul Kruger (1825–1904) of the Transvaal was overweight but not obese, although some British cartoons during the Boer War exaggerated his size.
A 2001 study by A. R. Walker, F. Adam, and B. F. Walker of the Human Biochemistry Research Unit, Department of Tropical Diseases, University of the Witwatersrand, South Africa, showed the general level of obesity in rural South Africa, Botswana, Namibia, and Zimbabwe remaining very low-between one and five percent. However, in urban areas, it became much higher, reaching eight percent in Cape Town for men and 34 percent for women. In South Africa, people suffering from obesity had a much greater likelihood of facing problems from arthritis, diabetes, and heart disease. his has led to an increased awareness campaign run by the Southern African Society for the Study of Obesity which has Professor Tessa van der Merwe of Netcare Bariatric Centres of Excellence, Unitas Hospital, Lyttleton, Pretoria, being the national representative on the International Association for the Study of Obesity.

{kind=link}