This is a worry with large strokes, such as big MCA strokes involving the basal ganglia, often with some involvement of the ACA or PCA territories as well, and large cerebellar strokes.
It is a worry with young patients who do not have much atrophy and thus not much room for the brain to swell inside the skull.
Monitor for any neurologic change, decline in level of consciousness, rising blood pressure, periodic breathing, hiccups, headache, new cranial nerve abnormalities, and pupils (late phenomenon).
Medical Treatment
. Most important is good post-stroke care such as head positioning (<158º), immediate correction of fever, electrolyte imbalance, and hyperglycemia, and careful optimization of MAP and cardiac output to insure adequate cerebral perfusion.
. Do not give steroids (grade A recommendation). Randomized studies have shown that steroids may be harmful rather than beneficial after acute stroke.
. Osmotherapy (i.e., mannitol) is a temporizing measure that may help in some cases. Give mannitol (0.5–1 g/kg bolus over30–60 minutes, and then 0.25 g/kg every 6 hours) aiming to increase baseline serum osmolality by 10%, but no higher than 315 mosm. Check serum osmolality every 12 hours and hold mannitol if >315 mosm.
. Cerebrospinal fluid drainage by ventriculostomy may help if hydrocephalus is contributing to increase ICP.
Surgical Therapy
. Obtain neurosurgical consultation early.
. For large MCA infarcts, consider early decompressive hemicraniectomy. The skull is taken off (and put in freezer) and dural incision is made so that the brain can swell out rather than compress the brainstem (see below). . For cerebellar stroke, the appropriate treatment is posterior fossa decompression and cerebellectomy.
. With both procedures, a common error is not to remove enough bone, resulting in inadequate decompression. Be sure the neurosurgeon knows the anatomical guidelines for decompression.
Decompress surgery is a life-saving measure. While it has never been proven effective in a randomized study, most stroke experts recommend it in highly selected cases based on case series. It is particularly recommended for large cerebellar strokes, as people can be quite functional without a large part of their cerebellum.
However, with respect to large MCA strokes, talk with family about quality of life after stroke survival versus death. Many do not perform the procedure as often for large left MCA strokes as the patient is likely to be left aphasic. Age is an important predictor of outcome after hemicraniectomy, all other things being equal, with less likelihood of acceptable outcome in patients over 60 years old.
Best results occur with early intervention in young patients with nondominant-hemisphere strokes.
Criteria for consideration of hemicraniectomy
. <5 hrs from onset; >50% MCA territory hypodense
. <48 hrs from onset; complete MCA territory hypodense
. >7.5mm midline shift
. >4mm midline shift with lethargy
Other criteria include:
– Age <60
– 145 cc infarct volume on MRIGuidelines for adequate surgical decompression from ongoing clinical trials
Guidelines for adequate surgical decompression from ongoing clinical trials
. Anterior: frontal to mid-pupillary line
. Posterior: 4 cm posterior to external auditory canal. superior: superior sagittal sinus
. Inferior: floor of middle cranial fossa
. Durotomy over the entire region of decompression
. Dural grafting
Other criteria include:
-12cm diameter craniectomy
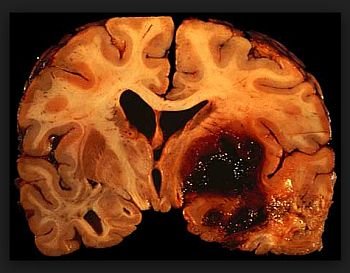
Hemorrhagic transformation
This should be clearly visible on non-contrast head CT. Most of the time, the patient is asymptomatic from the hemorrhagic transformation (also known as hemorrhagic conversion), unless it is large or in a critical location.
Radiographically, hemorrhagic transformation is divided into four categories.
. Hemorrhagic infarct 1 and 2 (HI1 and HI2) represent petechial bleeding into the area of infarct without mass effect and are rarely symptomatic. HI1 are small petechiae. HI2 are confluent. If HI occurs, usually there is not much you can do or should do, except to stop antiplatelets and anticoagulants temporarily until you are sure there is no continued bleeding on repeat brain imaging.
. Parenchymal hemorrhage 1 and 2 (PH1 and PH2) represent confluent bleeding. If the bleeding takes up more than 30% of the infarcted area and produces mass effect (PH2), it usually produces neurological deterioration.
The risk of developing PH2 is the main reason why anticoagulation is not recommended immediately after cardioembolic stroke, and without repeat brain imaging first. These should be managed similarly to any other cerebral hemorrhage