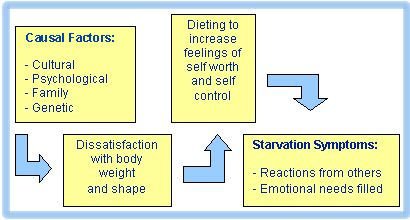
What cause anorexia nervosa?
This is perhaps one of the most frequently asked questions about anorexia and eating disorders. It is natural, of course, for patients, families, and loved ones to find themselves asking, “how did this happen?”Anorexia Nervosa, among the most serious of mental disorders, can be deadly for young women who get caught up in the malignant cycle of weight loss and compulsive behaviors. . . .
Researchers have spent more than a century trying to answer this important question. What they have determined is that there is no single cause of the illness. Instead, we now know that a combination of factors can contribute to the development of an eating disorder. The presence of these risk factors can increase a person’s vulnerability to anorexia, and, when combined with triggering life events, they may increase the likelihood of developing the disorder.
Each of the following factors has been shown to contribute to a person’s overall risk of developing anorexia nervosa. However, a person can develop anorexia without the presence of any of these risk factors. Alternatively, not everyone who evidences these risk factors goes on to develop anorexia. Instead, it is more likely that an interaction between various risk factors and life stressors make up a person’s overall risk profile. One important note: Knowing the cause of an eating disorder is not a prerequisite for getting help! Even if you are unaware of particular risk factors that apply, do not delay getting help for yourself or for a loved one.
An interaction between various risk factors and life stressors make up a person’s overall risk profile.
Genetic and Biological Risk Factors
Scientific studies have shown that some individuals may have a genetic predisposition toward developing an eating disorder, with some research indicating a hereditability factor greater than 50%. Multiple genetic influences (rather than a single, specific gene) appear to combine with environmental factors and lead to an increased risk for the illness. Studies show that people with a family history of anorexia are up to 12 times more likely to develop anorexia. Additionally, studies of identical twins with anorexia also point to a genetic predisposition for the illness. Note, however, that not every anorexia patient has a family history of eating disorders. According to the University of Maryland Medical Center, only about one-fifth of those with anorexia have a relative with an eating disorder.
Another area of biology that is important in understanding anorexia risk is brain chemistry. Scientific investigations have shown that the regulation of certain brain chemicals, called neurotransmitters, play an important role in certain psychiatric illnesses, such as depression and anxiety disorders. While we are just beginning the search into the role these chemicals may play in anorexia, there is increasing evidence that suggests neurotransmitters are a contributing factor in the course of anorexia. Some of the same neurotransmitters that influence aspects of mood and behavior (including serotonin, nor epinephrine, and dopamine) are being investigated as keys to understanding anorexia.
A technique called neuroimaginghas allowed scientists to examine the influence of these brain chemicals on human behavior, as well as upon sensations such as hunger and thirst. Neuroimaging was also involved in another recent discovery that revealed female anorexia patients have differences in a part of the brain called the insula, an area important in recognizing taste and responding to pleasure associated with food. Using functional magnetic resonance imaging (fMRI) to measure the brain’s reaction to taste, researchers from the University of Pittsburgh and the University of California, San Diego, found that individuals with anorexia process taste in a different way than those without an eating disorder.
Multiple areas of biological research have yielded additional advances in the understanding of anorexia. For example, certain digestive hormones (e.g., leptin and ghrelin) have been found at abnormal levels in anorexia patients. Also, it appears various hormones released in the body during times of stress may play a role. Recent research published in the Archives of General Psychiatry further suggests prenatal conditions may influence the likelihood of developing anorexia. Thus, as you can well imagine, the biological aspects of anorexia are complex, and research in this area is still in its infancy. We are continually learning more about the interaction between biological and genetic components with other factors that may contribute to the development and course of anorexia.
Experts are encouraged by recent research that has lead to the definitive understanding that anorexia is a biological, as well as a behavioral, illness. Thomas Insel, MD, Director of the National Institute of Mental Health conveyed that understanding when he made this landmark statement in October, 2006:
Anorexia Nervosa, among the most serious of mental disorders, can be deadly for young women who get caught up in the malignant cycle of weight loss and compulsive behaviors. . . . Research tells us that anorexia nervosa is a brain disease with severe metabolic effects on the entire body. While the symptoms are behavioral, this illness has a biological core, with genetic components, changes in brain activity, and neural pathways currently under study. (emphasis added) As our understanding of anorexia continues to advance, we find that research not only helps to clarify the nature of this illness but also provides critical support for continued healthcare research and the development of more effective means of treatment.
Developmental Factors
Although anorexia can occur throughout the lifespan, the most common period of onset is adolescence. Developmental changes that occur with puberty can increase a youth’s attention to, and dissatisfaction with, his or her body image. For both boys and girls, the interaction of pubertal hormonal changes, body preoccupation, and experimental dieting can interact to increase vulnerability to anorexic behaviors. However, while boys tend to gain muscle and lose fat at puberty, girls experience a normal increase in body fat, which is necessary for menstruation to occur. This natural increase in body fat may be perceived by some as “getting fat,” resulting in attempts at weight control or weight loss. Several studies indicate girls who experience early puberty are at greater risk for an eating disorder.
Peer factors during adolescence may also contribute to anorexia risk. Boys and girls who experience teasing about appearance and weight have been shown to be at greater risk for
eating disorders. Sexual anxieties, unwanted sexual advances, and/or sexual assault have been reported in a significant number of teens with anorexia. Studies suggest peer weight-loss behaviors and dietary restriction among close friends can also have an influence on attitudes about food and weight in adolescents and young adults. Life transitions within this stage of development, such as starting high school, the onset of dating, or leaving home to go to college, may interact with other risk factors to trigger eating disorder behaviors in vulnerable individuals.
Research tells us that anorexia nervosa is a brain disease with severe metabolic effects on the entire body.
Psychological Factors
Multiple psychological factors may contribute to the onset of anorexia. For example, anorexia patients have reported certain general characteristics such as low self-esteem, feelings of inadequacy, anger, guilt, and loneliness. More specific findings include those from a series of studies that revealed two factors distinguishing anorexia patients from other study participants: negative self-evaluation (thinking negatively about oneself) and perfectionism (Fairburn et al. 1999).
Certain personality traits have commonly been observed in anorexia patients, though it is important to note that there is no “personality formula” for understanding anorexia, nor is a patient’s personality to blame for their illness. Additionally, we are not be able to discern within some research results which observed behaviors may have been a precursor to the development of anorexia and which arose after the onset of the illness. With these caveats in mind, common characteristics have been observed in anorexia patients.
These include:
• Perfectionism and extreme conscientiousness
• Fearful or anxious temperament
• Drive for thinness
• Excessive control of emotions
• Sense of personal ineffectiveness or inadequacy
• Difficulty identifying or describing their own feelings
• Obsessive tendencies
• Extreme compliance to the demands of others (an extreme “people pleaser”)
• “Harm avoidance” (not wanting to upset anyone by their own behavior)
• Negative body image
• Maturity fears (fears about growing up to adulthood)
• Extreme shyness or social anxiety
• Cognitive inflexibility (rigidity in thinking; “all-or-nothing” thinking)
• Identity concerns
• Social isolation or fear of intimacy
To be clear, no single trait listed here is considered a direct cause for anorexia, nor do all individuals who evidence these traits go on to develop the illness. Rather, it is likely that certain personal characteristics, when combined with other risk factors, may increase one’s vulnerability to eating disorders.
Other psychological factors that may increase vulnerability are:
• A history of, or a co-occurring, psychological disorder
• Past experience of a traumatic event
• Emotional or interpersonal conflict
• Physical or sexual abuse
• A history of weight concern or childhood obesity
• Childhood feeding problems
• The effects of chronic illness
Occupational Factors, Athletics, and Other Activities
Studies show certain activities that include an emphasis on slenderness or weight control are associated with a higher risk for anorexia. For example, the prevalence rate of anorexia nervosa in ballet dancers is 4 to 25 times higher than that of the general population (Walsh and Cameron 2005). Other sports such as gymnastics, figure skating, wrestling, rowing, swimming, jockeying, track and field, and bodybuilding can involve certain weight restrictions that may lead to unhealthy attempts at weight control. Models and entertainment personalities may also experience social and occupational pressures to be thin. The more a person is involved in these types of activities, especially at advanced levels, the more likely they are to experience pressure about body shape and weight.
Familial Factors
Over the past several decades, certain commonalities with regard to family considerations have been noted in eating disorders literature. Many of these speculations have gone unsupported by scientific study, while others have proven to have some validity. One point that deserves emphasis is that the family does not cause anorexia. Rather, the familial component of a person’s experience is another area that can be important in understanding the overall picture of a person’s issues with weight and food. To be sure, the way parents interact with their children can have an impact on their emotional development.
Yet there is no “type” of family that causes anorexia and, as is true with individual psychological characteristics, we do not know for sure if certain family dynamics are present before an eating disorder develops, or in response to them.
Here is what we do know: There is a greater risk of someone developing anorexia when another member of the family has had an eating disorder.
This may be due to genetic influences and/or learned behavior within the family environment. For example, parents who have body image issues or unhealthy eating habits of their own may unwittingly make negative comments about weight and appearance that can influence other members of the family. We also know that people who feel less secure or unsafe in their family environment may be at greater risk for an eating disorder. For example, a family history of alcohol or substance abuse, physical, emotional, or sexual abuse, mental illness, or high parental conflict have been shown to increase risk.
There is greater speculation, however, about the role of other family characteristics in overall anorexia risk. For example, it has been suggested that parental indifference, extreme over-protectiveness, excessive performance demands, and emotional rigidity may be potential risk factors for a variety of mental illnesses and emotional distress; while compassion, acceptance, encouragement, and nurturing have been associated with greater resilience.
Dieting and Weight Loss Factors
Studies show that most cases of anorexia are preceded by an episode of dieting those progresses to anorexic food restriction and self-starvation. Clearly, not all attempts at dieting lead to disordered eating; however, studies have shown that the risk of developing an eating disorder is higher in dieting than in non-dieting adolescent girls. For example, a 1999 study in the British Medical Journal reported that girls who were defined as severe dieters were 18 times more likely than non-dieters to develop an eating disorder within 6 months.
Additionally, according to the National Eating Disorders Association, 35% of “normal dieters” gradually progress to pathological dieting, and of those, 20–25% later progress to either sub-clinical or clinical eating disorders. Nonetheless, questions remain regarding the exact nature of the link between dieting and anorexia.
Does dieting serve as a trigger for anorexia? Is it dissatisfaction with one’s body, and not the act of dieting per se, which represents the greater risk? Does calorie restriction cause physiological changes that lead to eating pathology in at-risk individuals? Does dieting represent a true risk for anorexia, or is it merely an early symptom of the illness?
While the exact nature of the relationship between dieting and anorexia is still under investigation, researchers are certain it cannot be ignored.
Social/Cultural Factors
In addition to individual factors such as genetics, family experience, and personality factors, certain social and cultural factors may increase the risk of developing anorexia nervosa. For example, recent research suggests Western cultural influences may play a role in the overall picture of eating disorders risk. Central to this influence is the value placed in Western societies on appearance, beauty, and the pursuit of thinness. Some experts even go so far as to say the preoccupation with weight and body image displayed in anorexia patients is merely an “exaggerated reflection” of the ubiquitous pursuit of thinness that pervades our Western culture. Even the casual observer would agree that ours is a culture that values thinness. One can scarcely pass a magazine rack, turn on the television, or watch popular films without being bombarded with images and ideas that equate success, happiness, and social acceptance with the “thin ideal.”
Eating disorders experts believe cultural expectations such as these have a profound effect on the prevalence of anorexia in Western society. Indeed, anorexia is often referred to as a “culture-bound syndrome,” implying that prevalence of the illness is directly influenced by attitudes, values, and behaviors that are prized in Western culture.
Studies show anorexia nervosa is most prevalent in industrialized countries where dieting and the pursuit of thinness are the accepted norm. In contrast, non-Western countries report lower rates of anorexia. Researchers are finding that with globalization and Western influence comes the desire to emulate Western ideals, including ideals related to appearance and attractiveness. Results of a landmark study published in 1999 revealed a dramatic increase in the rate of eating disorders among teenage girls in the Pacific Island nation of Fiji that was linked to the introduction of Western television programming.
Harvard eating disorders researcher Anne Becker studied the eating habits of Fijian schoolgirls between 1995 and 1998, a period that marked the introduction of Western television programming to an otherwise traditional, agricultural society. There was only one TV station available, which broadcasted mostly American, Australian, and British favorites such as Seinfeld, ER, and Melrose Place. Becker reports that the proportion of students who scored high on an eating disorders risk evaluation rose from 13% to 29% in the 38 months that followed the introduction of TV programming. Those who watched TV at least 3 nights per week were 50% more likely to see themselves as “too fat” and 30% more likely to diet. Fifteen percent had reported they induced vomiting as a means of weight control, up from 3% shortly after the study began. Overall, symptoms of eating disorders among teenage girls increased fivefold in 4 years. A 2005 study of more than100 female international students from Japan, China, Taiwan, and Hong Kong found that a greater acceptance of a Western ideal of thinness was associated with greater eating disorder symptoms.
Likewise, a 2007 study published in the Journal of Nervous and Mental Disease found that media exposure and travel abroad was correlated with eating disorder symptoms in females from the East African country of Tanzania. Additional studies reported in the International Journal of Eating Disorders reveal that as adolescents from more weight-tolerant countries become assimilated to Western culture, they report more fear of weight gain and an increase in symptoms of disordered eating.
Cultural influences of a social nature may also contribute to the increased risk of anorexia among females. According to the Clinical Manual of Eating Disorders, the disparity in prevalence rates between male and female adolescents who develop anorexia has been attributed in part to the greater cultural pressures on young women to be thin. Researchers note that appearance is often a central factor to how females are valued in Western culture. Therefore, beauty and body image become more salient to a young woman’s self-esteem. In addition, researchers suggest anorexia may be a response to role-conflicts and complex pressures of socialization experienced by contemporary females.
A 2003 issue of Parade magazine included this comment about the cultural demands placed on women: “In order for a woman to consider herself happy, she has to be in a good relationship, be happy with her kids, her friends have to like her, her job has to be going well, her house has to look good, and she has to be thin” (emphasis added). Mounting social and cultural pressures may be just one more piece in the overall puzzle that determines eating disorders risk in vulnerable individuals.
Stress Factors and Emotional “Triggers”
Each of the factors discussed so far can influence an individual’s risk of developing an eating disorder. Yet eating disorders are also often precipitated by (or “triggered” by) an emotional life event or period of significant stress. Significant stress, when coupled with inadequate coping resources, can combine with other risk factors to increase a person’s vulnerability to illness.
Potential triggers for anorexia can include:
• Environmental changes (changes in school, moving to a new home or city)
• Family changes (parental divorce, birth of a child, increased familial stress)
• Loss of a loved one (through death or break-up of a relationship)
• Trauma
• Uncomfortable feelings about adult sexuality or unwanted sexual advances
• Maturity fears
• Increased familial responsibility and caretaking
• Dieting to promote weight loss (often for an upcoming special event)
• Industry pressure to maintain a certain physical appearance
• Teasing or being bullied
• Rejection
• Threats to physical safety or security
• Academic difficulties
• Peer pressure (including pressure from team sports)
• Chronic illness, especially one that may affect weight or appearance
• Other significant loss or disappointment
There is a greater risk of someone developing anorexia when another member of the family has had an eating disorder.
Thirty-five percent of “normal dieters” gradually progress to pathological dieting, and of those, 20–25% later progress to either subclinical or clinical eating disorders.
Terms:
Risk factor – A characteristic that increases an individual’s likelihood of developing an illness.
Genetic predisposition – An inherited genetic pattern that may make a person more susceptible to a disease or condition.
Hereditability factor – A calculation of the contribution made by genes to the causation of a disorder or disease.
Neurotransmitter – A chemical substance in the brain that facilitates communication between nerve cells.
Serotonin – A brain chemical thought to be important for regulating sleep, appetite, mood, and pain inhibition.
Norepinephrine – A neurotransmitter in the brain that is involved in the regulation of sleep, arousal, mood, and response to stressful stimuli.
Dopamine – A neurotransmitter which has been associated with the areas of the brain that regulate movement, mood, emotion, motivation, and pleasure.
Neuroimaging – Techniques that allow mapping of the structure or function of the brain.
Thin ideal – Cultural attitudes which imply that extreme thinness is a requisite for attractiveness. Such ideas may inadvertently promote unhealthy weight control methods in society-at-large by promoting conformity to an unrealistic “ideal” body shape and size.
Functional magnetic resonance imaging (fMRI) – A type of brain scan used to study activity in the brain. An fMRI shows which structures are active during particular mental operations.
Leptin – A protein hormone that helps the body regulate appetite and the metabolism of fats.
Ghrelin – A hormone that relays messages between the digestive system and the brain to stimulate appetite.
Prenatal – Occurring or existing before birth.
Anorexia nervosa is most prevalent in industrialized countries where dieting and the pursuit of thinness are the accepted norm.



{kind=link}