Drug Addicted Children Documentary
When should we consider residential programs for our daughter?
In cases where an adolescent needs long-term treatment, residential programs employing the principles of a therapeutic community (TC) can be considered. These are individuals with long-standing history of drug use, failed intensive programs, and those with legal problems. A number of adolescents are also court mandated to complete residential programs. There are also certain TC programs that incorporate psychiatric consultations to deal with treatment and diagnostic issues and also for medication evaluations. Some TCs are modified to meet the needs of special populations like mentally ill chemical abusers in community residences, adolescent substance abusers in residential TCs, and criminal offenders in corrections facilities.
The TC consists of staff with or without recovery experiences and provides a constellation of services including medical and mental health and vocational and educational services. Work and assigned job responsibilities are a means to therapy and improving interpersonal skills with both peers and authorities. Peers act as role models to expected behaviors. Staff members play the role of rational authority figures, providing feedback and direction.
Those in the program are expected to work with the “program,” which refers to following the structure and communication lines of the community and the “family” (clients and staff). The program follows a strict schedule of therapeutic, recreational, and educational activities.
Encounters are the cornerstone of treatment. These are peer led, and participants are made aware of the behaviors that need to be modified. Probes, on the other hand, are staff led, with the goal of further understanding the individual’s background for treatment planning purposes and also for fostering trust, openness, and support. Some have even claimed that residential treatment does not work. To simply view residential treatment as a failure is to overlook a number of factors that have been identified that affect long-term outcomes, both positive and negative, and the corrective actions that have been incorporated by providers to directly address this gap.
Because 60% of individuals relapse within 90 days of discharge from residential treatment, case management, coupled with assertive interventions, was designed to provide rapid initiation of continuing care in the community. This is part of the discharge planning that is done while still in treatment.
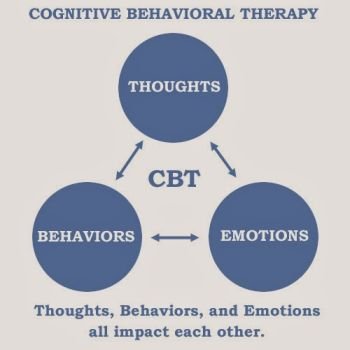
An important aspect of any treatment is to establish support that such interventions do in fact work when using clearly defined outcome measures. In the substance abuse field, there are a number of evidence-based interventions including Cognitive Behavior Therapy (CBT), Motivational Enhancement Therapy (MET), Community Reinforcement
Approach (CRA, adapted for adolescents), and Contingency Management (CM). CRA is a comprehensive behavioral approach aimed at identifying factors in the environment that promote sobriety. It also involves skill building and developing pro social skills that compete with drug-seeking behaviors. CM is differentially rewarding desired behaviors (sobriety) while punishing or withholding reinforcement for undesired behaviors (drug use). Positive reinforces can include receiving vouchers or tokens if abstinence is exhibited and being placed on contract, bracelet monitoring, or house arrest for drug relapse. The challenge is for these proven treatments to be provided at varying levels of care from the traditional out patient to day programming to levels as intensive as an inpatient setting or a residential program.
In a recent study (Garner et al., 2009), the Washington Circle (WC) continuity of care after long-term residential treatment performance measure was studied as well as the effect of assertive continuing care interventions in achieving continuity of care. The WC, which has been previously shown to be reliable with patients, was now tested to see if it can be generalized to a program level (residential treatment facility) whose treatment is reimbursed through public funding. Three hundred and forty-two adolescents who were admitted to long-term residential treatment were randomly assigned to either standard continuing care or an assertive continuing care condition (CRA, CM, or both). Because the study utilizes a randomized design, it experimentally tested the ability of the WC performance measure to predict outcome.
The following were measured: degree of substance related problem, length of residential treatment, type of intervention, whether the intervention was with or without assertive conditions, presence or absence of follow-up within a two-week period after discharge from residential treatment, and recovery status (whether sober or not) while in the community.
Individuals included in the study were mostly adolescent Caucasians between 15 and 16 years old with significant legal involvement, high levels of dependence (mostly to cannabis and alcohol), and high co-occurring psychological problems and involvement in risky behaviors (multiple sexual partners and unprotected sex).
Those adolescents involved with WC have a significantly higher continuity of care treatment. Greater severity of the substance problem at baseline decreases the likelihood of recovery at three months. This emphasizes the need to provide ongoing effective substance abuse interventions by qualified and trained clinicians. Because there is a high degree of co-occurring psychological conditions, treatment also has to address these. Adolescents achieving continuity of care criteria had approximately a 92% chance of being sober at three-month follow-up compared with adolescents who did not achieve these criteria.
There are component treatments that do work. What is important is to provide these services concurrently in a coordinated manner from a multimodal and multidisciplinary approach and where case management is also provided. Meeting the needs of the adolescent should be guided by what can minimally meet his or her needs given a particular set of circumstances. Residential treatment may well be the least restrictive level meeting the youngster’s needs at a particular time and this certainly needs to be periodically reviewed and revised accordingly as to whether criteria for this level of care are continually met.
I’ve heard about 12-steps programs. Are they for adults only?
Most Alcoholics Anonymous (AA) and Narcotics Anonymous (NA) groups are for adults, and adolescents may be unable to identify with what is going on in the meetings. Parents have even expressed concern that their sons and daughters will be influenced by hard-core drug addicts there. While these concerns can be valid, they illustrate that it is all the more important that parents help find the right fit for their children. The utility of these support groups can be more meaningful for adolescents who have already been introduced to them in prior treatments. Most of the interventions are provided in longer term treatments. The 12-steps programs are rooted in the belief that recovery from addiction is only possible if one recognizes his problem with alcohol or drugs and admits that use of drugs in moderation is impossible without significant psychosocial consequences.
The most widely used approach is based on the principle and philosophy of AA and NA. Treatment programs based on NA/AA models are also known as the
to five steps during inpatient or residential treatment. Concepts of acceptance, surrender, spirituality, and powerlessness may be difficult for adolescents to handle. The Step Workbook for Adolescent Chemical Dependency Treatment (Jaffe, 1990) offers a developmentally appropriate guide to the first five steps. Step 1 is the acknowledgment of inability to control substance use and is a confrontation of denial as well as developing motivation to participate in treatment. Steps 2 and 3 are also motivational in nature, emphasizing the need for help from someone other than the addict himself or herself. Adolescents are encouraged to look outside of themselves for guidance, structure, and meaning. Step 4 is the development of moral inventory involving a description of past behaviors. This lays the groundwork for subsequently dealing with issues identified. Step 5 explicitly asks for verbal disclosure and implicitly letting the adolescent deal with a helping individual. This modified approach still needs to be empirically tested.
Adolescents are encouraged to look outside of themselves for guidance, structure, and meaning.


{kind=link}