Open Prostatectomy for Benign Prostatic Hyperplasia
Surgical Treatment of Benign Prostatic Hypertrophy
What is an open prostatectomy?
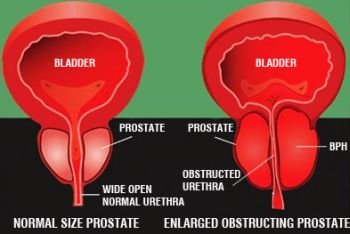
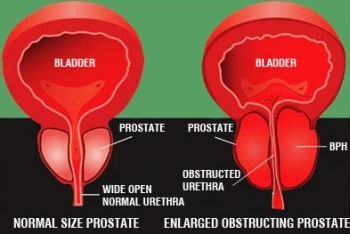
An open prostatectomy refers to the removal of the obstructing portion of a benign prostate through a surgical incision. Open prostatectomies are usually reserved for large prostates that weigh over 100 grams.
The most common approach to perform an open prostatectomy is through a lower abdominal incision that extends from the symphysis pubis to the umbilicus (belly button).
After the surgeon enters the abdomen through this incision, he or she has two surgical choices. The first is to make an incision in the anterior (front) wall of the bladder to approach the prostate. This is called a suprapubic prostatectomy. After the surgeon has entered the bladder, he or she can enucleate or shell out the center of the prostate with his or her index finger.
After the inner portion of the prostate is enucleated, stitches are placed in the prostatic fossa (the shell of prostate that is left). Postoperatively, the patient is left with a urethral catheter coming out of his penis and a suprapubic catheter coming out of the lower abdomen.
A patient is usually in the hospital 3 or 4 days after a suprapubic prostatectomy.
A retropubic simple prostatectomy is similar to a suprapubic simple prostatectomy as it is also performed through a lower abdominal incision.When performing a retropubic simple prostatectomy, however, the urologist does not open the bladder but instead makes an incision through the prostate capsule. As is done with a suprapubic prostatectomy, the inner portion of the prostate is shelled out or enucleated. Because the bladder is not opened, it is not necessary to leave a suprapubic tube postoperatively, but a urethral catheter is left in place.
Like a suprapubic simple prostatectomy, the patient is usually in the hospital 3 or 4 days postoperatively. In addition to the abdominal approaches described previously here, a benign prostate can be surgically approached via the perineum. The perineum is the area between the scrotum and the anus. When this approach is used, the perineal skin incision is used to expose the prostate; then an incision is made in the prostatic capsule, and the prostate is enucleated, similar to a simple retropubic prostatectomy. A urethral catheter is left postoperatively, and the patient is usually in the hospital 1 to 2 days.
What is a transurethral prostatectomy?
A transurethral prostatectomy (TURP) is an operation that is designed to remove the prostate through the urethra; no external incision is made. A TURP is performed using a special instrument called a resectoscope, which scrapes out the center of the prostate by using an electrical current that cuts out the tissue with a loop. In order to permit transmission of the electrical current from the loop to the tissue, the irrigating fluid normally used for a TURP is a glycine solution. This solution is somewhat more dilute than blood, and if the resection lasts a prolonged period of time, more than one hour, the patient can absorb too much fluid through the resected prostatic tissue bed and become hyponatremic (a low serum sodium). In severe cases, hyponatremia can cause neurologic symptoms, including seizures. Fortunately, these complications occur vary rarely. TURPs are usually limited to prostate glands of 100 grams or less.
After the TURP has been completed, a urethral catheter is left to enable irrigation of the bladder with fluid, typically for 1 to 2 days. After that period of time, the catheter is removed, and the patient is given a voiding trial.
JN: Can the Targis procedure be used on a patient who has had a TURP?
KL: Yes, it can.
What is a transurethral incision of the prostate?
A transurethral incision of the prostate (TUIP) is exactly that, an incision rather than a resection of the prostate. The technique of a TUIP is to use a special knife-like instrument called a Colling’s knife that is placed through the same resectoscope sheath that is used for TURPs. Electrical current is transmitted through the knife, and two incisions are made at 5 o’clock and 7 o’clock through the bladder neck and prostate to the verumontanum where the ejaculatory ducts exit. The verumontanum is a landmark for the external sphincter, and the urologist does not want to cut beyond that.
A TUIP as opposed to a TURP is a quicker, easier procedure. TUIPs tend to be used in younger men with smaller prostate glands. The incidence of retrograde ejaculation after TURP ranges from 50% to 95%, whereas the incidence is from 0% to 37% with TUIP. In properly selected patients, those with small glands, the rate of symptom relief with TUIP approaches that of TURP.
JN: If a man experiences problems with impotency after undergoing a TURP or TUIP, can those problems be corrected later?
KL: Postprostatectomy erectile dysfunction can be treated with a variety of medications or surgical implants.
Terms:
Open prostatectomy – a technique to remove the prostate through a skin incision.
Suprapubic prostatectomy – removal of a portion of the prostate through a lower abdominal incision.
Perineum – in a male, the region between the scrotum and rectum.
Transurethral – prostatectomy a method of removing obstructive prostate tissue through the urethra so that no external incision is made; also known as TURP.
Resectoscope – an instrument used to remove (resect) prostate, bladder, or urethral tissue through the urethra.
Hyponatremic – a low sodium level in the blood.

{kind=link}