Jennifer Lawrence on Body Image
Sometimes I have an extremely difficult time communicating my emotions. Could this problem be related to my anorexia?
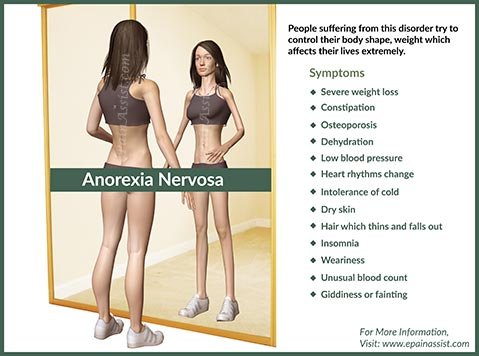
You may be referring to alexithymia, a trait characterized by the inability to identify and describe emotions, confusion about one’s own feelings, and/or an apparent lack of consideration about one’s own personal experiences. Literally translated, the word alexithymia means “absence of words for emotion,” a fitting description for those who experience it. Although people with alexithymia experience the expected physical responses associated with emotions, such as changes in heart rate, or even tears, they are typically unable to connect these reactions to their underlying emotions. Moreover while some people with alexithymia may be able to express that they feel certain sensations, such as sadness, fear, happiness, or anger, they are typically unable to connect these sensations to a particular event or circumstance. Alexithymia is not the same thing as apathy, denial of emotion, or a lack of concern for others. However, a person with alexithymia may appear emotionally detached and may have difficulties connecting to others.
Studies show that rates of alexithymia are higher among those with eating disorders than among the general population. Research published in Comprehensive Psychiatry reported that approximately 40–68% of eating disorder patients experience some degree of alexithymia. Alexithymia is also common among people with depression and certain types of anxiety disorders. While more research is needed, the inability to regulate uncomfortable emotions coupled with a lessened ability to experience positive emotions (both are associated with alexithymia) may contribute to the overall risk of developing anorexia.
The causes of alexithymia are still under investigation. Some studies indicate that alexithymia may be due to a disturbance in the right hemisphere of the brain, an area largely responsible for processing emotional cues. Other studies suggest a decreased ability for neural communication between the various regions of the brain involved in translating emotional cues and expressing emotions. Some researchers have looked at the importance of parental response to their children’s emotions and the effect this may have on a child’s natural range of expressing emotion.
Healthcare professionals typically assess for alexithymia using an inventory called the Toronto Alexithymia Scale-20, which measures three core features: difficulty identifying feelings, difficulty communicating feelings, and externally oriented thinking. This brief screening tool can help determine the degree to which alexithymia may affect treatment and recovery from anorexia. Problem solving therapy and Dialectical Behavior Therapy are two therapeutic approaches that have shown promise with alexithymia. Alexithymia can pose a challenge to recovery, especially if it goes unnoticed, so be sure to talk to your healthcare professional if you experience any of the following signs of alexithymia:
• Difficulty identifying and/or verbalizing different types of feelings
• Difficulty distinguishing between emotional feelings and bodily sensations
• Limited understanding of what causes unique feelings
• Limited fantasy thinking or emotional content of imagination
• Lack of enjoyment and pleasure-seeking
• Often perceived by others as excessively logical, or unsentimental
• Often confused by others’ emotional reactions
Sarah shares:
Even to this day, I sometimes find myself using food restriction or compulsive exercising as a distraction from the bigger issues in my life. When emotional events occurred in my life that I had no control over, I subconsciously turned to my eating disorder to give me the sense of control I was lacking. Everyone has his/her coping mechanisms for dealing with unpleasant times; mine was just extremely dangerous and unhealthy.
I’ve learned now to recognize when I am using food or exercise as a coping mechanism, and I have a number of other, much more helpful and fulfilling ways to deal with the stress that life brings.
Term:
Externally oriented thinking – Thinking that tends to focus on external events rather than inner emotional experiences.
Approximately 40-68% of eating disorder patients experience some degree of alexithymia.
I recently noticed that my sister has scars on her arms and wrists. I am concerned that she may be intentionally hurting herself. Why would she do this?
Certainly, it can be disturbing to know that a loved one may be engaging in this form of behavior. While these behaviors may strike you as being highly unusual and may indeed be quite troubling, you should know that self-injury is becoming increasingly common among eating disorder patients. Approximately 25% of people with an eating disorder engage in self-injurious behaviors. The risk increases with the presence of certain co-occurring mood and personality disorders. Self injury (also called self-mutilation, self-harm, or self-abuse) is defined in the Journal of Clinical Psychiatry as behavior involving the deliberate infliction of physical harm to one’s own body without any intent to die as a consequence of that behavior. In other words, self-injury is not necessarily an attempt at suicide, although that possibility should always be considered (if your loved one’s behavior raises concerns for his or her immediate safety, contact 911 or bring your loved one to a local emergency room for evaluation). Examples of common modes of self-injury include hair-pulling, skin-cutting, head-banging, skin-picking or scratching, biting, hitting, or burning. Often, patients who engage in self-harm may injure themselves on areas of their body that are less visible (such as their shoulders, upper arms, or thighs), or they may try to cover any residual scarring in an attempt to conceal their behavior; however, attempts at secrecy are often unsuccessful. What motivates a person to self-injure? Usually, and perhaps not surprisingly, patients may self-injure as a means of coping with very uncomfortable emotions. People who self-injure report extreme feelings of tension, anxiety, stress, or emotional pain just before harming themselves. Patients sometimes see self-injury as a way of distracting themselves from that pain or “releasing it” in an attempt to self-soothe; many report that self-injury makes them “numb” to their emotions, bringing them a sensation of peace or temporary relief. Conversely, some patients who self-injure report feeling “dead inside” and “numb” to emotional states. In these cases, self-injury becomes a means of reminding themselves that they are “alive on the inside.” Self-harm can also be a form of self-punishment for behaviors that bring shame or guilt. Self-injury is often a vicious cycle, given that the perceived relief is only temporary and does not represent a means for dealing with the underlying issues. In fact, the shame that people feel after harming themselves may lead to additional attempts at self-harm.
The cycle of self-injurious behavior may yield an increased sense of desperation, potentially involving attempts at suicide. Therefore, self-injurious behavior should always be taken seriously. Indeed, studies show that the risk of suicide is a serious and substantial concern for patients with anorexia nervosa. Research indicates that approximately 25% of anorexia related deaths are due to suicide and that patients with anorexia often use extremely lethal methods when attempting suicide, indicating a strong wish to die. Therefore, anorexia patients should be monitored closely for suicide risk. Factors that may increase the risk of suicide are age at onset of anorexia, longer duration of the illness, lower body weight, certain co-occurring psychiatric disorders, and substance abuse. Additionally, recent studies have suggested that patients who take certain antidepressant medications should be monitored for increased risk of suicidal thinking and suicidal behavior; this is particularly a consideration for children and adolescents.
If your loved one shows signs of self-injury, please encourage them to get help. At the very least, self-injury represents a threat to an individual’s overall well-being and quality of life. The reality is that self-injury can cause more harm than intended and can result in serious medical complications, or even death. A healthcare professional can help determine the immediacy of risk in your loved one’s situation and assess the need for intensive treatment or hospitalization. Remember that self-injurious behavior may be one of the only ways your loved one knows how to cope with their feelings of distress, so try not to judge, blame, or criticize them for their behavior. Express your concern for their well-being, and let them know that you want to help. If you do not feel comfortable talking to them about their self-injuries, be honest about your limits. The important things are to let your loved one knows of your concern and to point them toward help and appropriate care. Approximately 25% of people with an eating disorder engage in self-injurious behaviors.



{kind=link}