VIDEO
Obesity and Diabetes: Twin Epidemics of the 21st Century
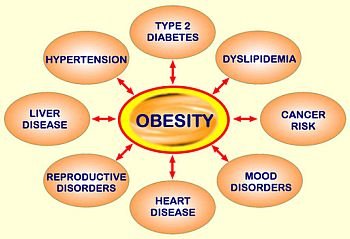
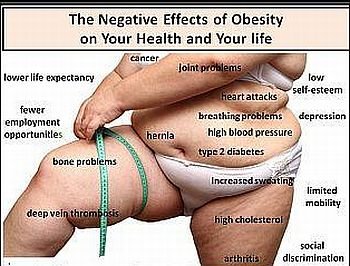
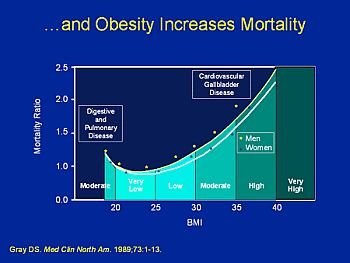
Health Risks of Overweight and Obesity
Morbidity
Dyslipidemia,
The Dyslipidemia is manifested by:
Diabetes Mellitus
The increased risk of diabetes as weight increases has been shown by prospective studies in
More recently, the Nurses’ Health Study, using data based on self-reported weights, found that the risk of developing type 2 diabetes increases as BMI increases from a BMI as low as 22. Since women in particular tend to underreport weight, the actual BMI values associated with these risks are likely to be higher than the Nurses’ Health Study data would suggest. An association between type 2 diabetes and increasing relative weight is also observed in populations at high risk for obesity and diabetes, such as in American Indians. In recent studies, the development of type 2 diabetes has been found to be associated with weight gain after age 18 in both men and women. The relative risk of diabetes increases by approximately 25 percent for each additional unit of BMI over 22 kg/m2. In addition, in a prospective study representative of the
Coronary Heart Disease
Observational studies have shown that overweight, obesity, and excess abdominal fat are directly related to cardiovascular risk factors, including high levels of total cholesterol, LDLcholesterol, triglycerides, blood pressure, fibrinogen, and insulin, and low levels of HDL-cholesterol.
Plasminogen activator inhibitor-1 causing impaired fibrinolytic activity is elevated in persons with abdominal obesity. Overweight, obesity, and abdominal fat are also associated with increased morbidity and mortality from CHD. Recent studies have shown that the risks of nonfatal myocardial infarction and CHD death increase with increasing levels of BMI. Risks are lowest in men and women with BMIs of 22 or less and increase with even modest elevations of BMI. In the Nurses’ Health Study, which controlled for age, smoking, parental history of CHD, menopausal status, and hormone use, relative risks for CHD were twice as high at BMIs of 25 to 28.9, and more than three times as high at BMIs of 29 or greater, compared with BMIs of less than 21. Weight gains of 5 to 8 kg (11 to 17.6 lb) increased CHD risk (nonfatal myocardial infarction and CHD death) by 25 percent, and weight gains of 20 kg (44 lb) or more increased risk more than 2.5 times in comparison with women whose weight was stable within a range of 5 kg (11 lb). 90 In British men, CHD incidence increased at BMIs above 22 and an increase of 1 BMI unit was associated with a 10 percent increase in the rate of coronary events. Similar relationships between increasing BMI and CHD risk have been shown in Finnish, Swedish, Japanese, and

{kind=link}