Prostate cancer: Essential facts
Prostate Cancer: Causes, Symptoms and Treatments
Prostate cancer mortality statistics
What is prostatitis?
Prostadynia has symptoms that are indistinguishable from prostatitis. A generation ago prostadynia was essentially considered the same as nonbacterial prostatitis; however, today, most urologists agree that prostadynia is caused by a spasm of the bladder neck, prostatic capsule, or prostatic urethra, whereas nonbacterial prostatitis may be caused by Chlamydia trachomatis or similar infectious agents.
How is prostatitis diagnosed?
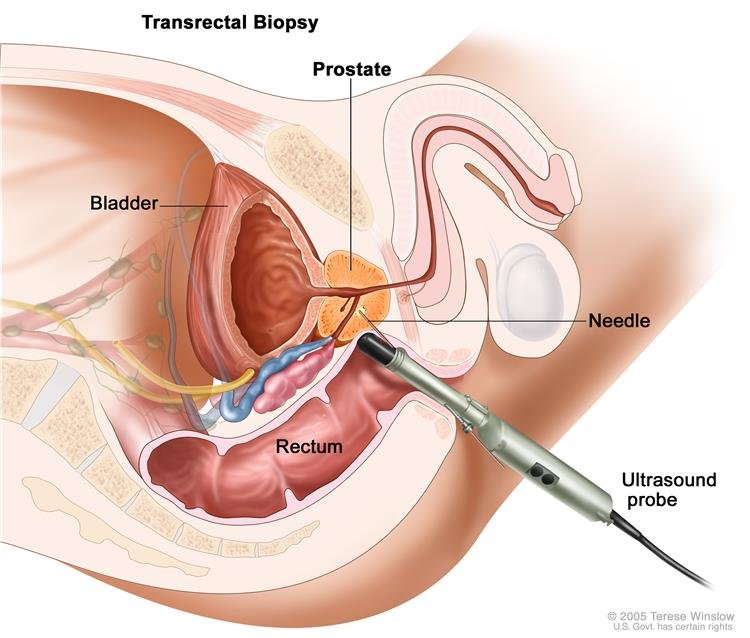
The classic diagnostic maneuver for bacterial prostatitis is the so-called three-glass test. The patient is asked to void and collect his first 10 ml of urine. This is sent for culture and is known as VB1. Then the patient is asked to collect a midstream urine sample after he voids about 200 ml. This urine sample is sent for culture and is known as VB2. Then the urologist performs a digital rectal exam and massages the patient’s prostate in an attempt to express prostatic secretions (EPS) into a sterile container. A prostatic massage is not always successful in producing sufficient secretions, and for some men, it can be quite uncomfortable. After the prostatic massage, the patient is asked to void again into a container, referred to as VB3, and this sample is sent for culture. If there is an increase in the number of bacterial colonies seen in either EPS or VB3, a diagnosis of bacterial prostatitis is made, and treatment is based on the antibiotic sensitivities of the organisms that were isolated.
How is prostatitis treated?
For most urologists, antibiotics are the first line of treatment for suspected prostatitis; however, the patient should recognize that if the urologist uses the three-glass test, many cases of prostatitis are treated empirically. In most cases of clinical prostatitis, a bacterial organism is not isolated. The urologist usually chooses an antibiotic that has pharmacokinetic properties that include good penetration into prostate tissue. Commonly used antibiotics for prostatitis include the sulfonamides and quinolones; however, the duration of time of antibiotic therapy also depends on the judgment of the urologist. It can vary from a week to months. Because much of the treatment of clinical prostatitis is empiric, if a patient does not respond to the initial antibiotic treatment, the urologist will often switch the patient to a different antibiotic and then monitor the patient’s clinical response.
Because the entity of nonbacterial prostatitis is also recognized and is often felt to be due to Chlamydia trachomatis, some urologists will give the patient a course of doxycycline, an antibiotic that covers Chlamydia particularly well.
How is prostadynia diagnosed?
Prostadynia is essentially a diagnosis of exclusion. If a patient is diagnosed with prostatitis, he will normally be treated with a course of antibiotics. If he does not respond clinically to the antibiotic, the urologist will usually either try another antibiotic or consider that the patient may have prostadynia. No objective clinical test or measurement is available that can be used to confirm a diagnosis of prostadynia. It is a clinical diagnosis made by the judgment of the treating urologist.
How is prostadynia treated?
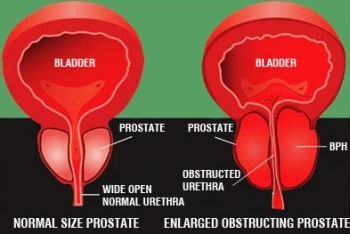
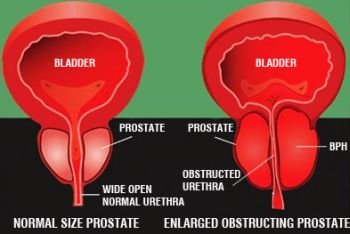
Because prostadynia is felt to be due to a spasm or increased neurologic tone of the prostate, the class of drugs known as alpha blockers is used to treat prostadynia. Alpha blockers are the same group of drugs that can be used to treat signs of prostatic obstruction in patients with BPH.
The urologist will use the clinical response of the patient to alpha blockers to determine the length of time to continue treatment. Several alpha blockers are available, but no single drug in this class has been shown to be superior to the others in the treatment of prostadynia.
Who gets prostate cancer?
Prostate cancer is a disease of middle-aged and older men. In 2013 in UK it is estimated that there will be 47,300 new new cases of prostate cancer diagnosed, and 11,287 men will die from prostate cancer. It has been estimated that one in eight white American men will develop prostate cancer in their lifetimes. The difference in prostate cancer rates differs markedly by race. The incidence of prostate cancer in African Americans approaches 90 per 100,000 per year, in Caucasians 40 to 60 per 100,000 per year, and in Asians 2 to 10 per 100,000 per year. Asian men who move to the United States at a young age have higher rates than Asian men who remain in their native environment. This suggests that dietary and environmental factors may influence the rates of prostate cancer as well.
Family history also plays a significant role in the development of prostate cancer. It is estimated that a man with a first-degree relative with prostate cancer has a 2.1- to 2.8-fold greater risk of developing prostate cancer than the general population. Diet also likely is important in prostate cancer development. High dietary fat content appears to confer a 1.6 to 1.9 times greater risk of prostate cancer development. There has been controversy in the literature as to whether smoking history, occupation, or socioeconomic status is linked to prostate cancer. To date, there is no conclusive evidence that any of these factors significantly impacts the risk of prostate cancer.
JN: Scientists have been learning more about the role of inflammation as a marker for various diseases. Is there any reason to believe that there are toxic agents that might cause a prostate to become inflamed and that this inflammation might cause an infection that would start the process of creating prostate cancer cells?
KL: The answer to this question is not known. Researchers are looking into the link between prostate infection and prostate cancer.

{kind=link}