Blood test ‘improves’ prostate cancer treatment’
Prostate cancer: Blood test could help target treatment
How is prostate cancer diagnosed?
Prostate cancer is diagnosed by a digital rectal exam and a PSA blood test. It has been shown that a digital rectal exam and PSA test together are superior to either examination alone. Controversy exists, however, among regulatory bodies whether men should be screened for prostate cancer.
Those agencies that do endorse prostate cancer screening recommend that all men obtain an annual PSA test and digital rectal exam starting at the age of 50 years and those in high-risk groups, African American men, or with a family history start getting PSAs and digital rectal exams at the age of 40 years.
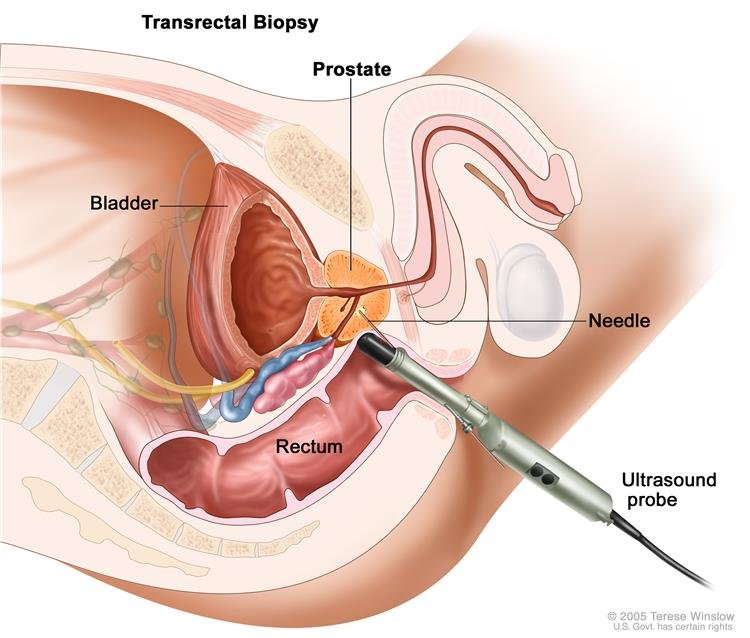
What are prostate ultrasound and biopsy?
A prostate ultrasound and biopsy are performed to obtain prostatic tissue to make a definitive diagnosis of prostate cancer.Without a tissue diagnosis, one cannot be sure that an individual man has prostate cancer regardless of his rectal exam or PSA level.
A prostate ultrasound and biopsy are usually done in the urologist’s office. A patient typically will be asked to take antibiotics either before or after the biopsy depending on the individual urologist’s custom. Many urologists also ask the patient to refrain from aspirin for 10 days before the biopsy to minimise the risk of bleeding and to administer a Fleet enema to himself the night before or morning of the biopsy to clean out the rectum. The urologist may perform the ultrasound and biopsy by himself or with a radiologist or ultrasound technician.
The patient is asked to lie on his side with his knees pulled up to his chest. Lubrication is placed in the rectum and an ultrasound probe, which is a plastic tube about the width of two fingers, is then placed in the rectum. This ultrasound probe transmits a picture of the prostate on to a screen where it is viewed by the urologist. Many urologists will then inject a local anaesthetic into the surface of the prostate to numb the prostate before the biopsies are taken.
At this point, a spring-loaded biopsy gun is placed through a channel in the ultrasound probe. The biopsy gun takes small cores of tissue from the prostate. The number of cores taken is variable and depends on the judgment of the urologist. The prostate cores are sent to pathology for review and diagnosis. The typical ultrasound and prostate biopsies take 20 to 30 minutes. The patient is sent home with oral antibiotics, and the patient may see blood in his urine, stool, or semen for several days or at times for several weeks after the biopsies.
JN: Do negative results of a needle biopsy mean that the patient’s prostate is free of cancer or that just the portions of the prostate that were selected for biopsy were free of cancer or that the cancer was so small that the biopsy made it difficult to identify?
KL: A negative biopsy does not categorically prove that the patient does not have cancer. Sampling error can occur and small tumours can be missed. Therefore, follow-up after a negative biopsy is important.
What are Gleason grades and scores?
For many years, pathologists described the histologic (microscopic) features of prostate cancer in a very imprecise way. Pathologists generally lumped prostate cancer into one of three categories: well, moderately, or poorly differentiated tumours. Then, in 1974, Donald Gleason, a pathologist at the University of Minnesota, published a set of reproducible criteria that pathologists could use to describe or grade prostate cancer. The grades ranged from 1 through 5, with 1 being the best or least aggressive cancer and 5 being the worst or most aggressive cancer.
A Gleason score is calculated by adding together the two most prevalent grades in the tissue that the pathologist examines. Therefore, the best Gleason score is a 1 + 1 = 2, and the worst is a 5 + 5 = 10.
If the tumour is not homogenous, then the most prevalent grade is listed first, such as 5 + 4 = 9. It should be emphasised that a Gleason score 4 + 3 = 7 is different than a 3 + 4 = 7 because the most prevalent grade is higher. Almost all pathologists who examine prostate cancer now use the Gleason scoring system.
Is prostate cancer genetic?
To some degree prostate cancer is genetic. Prostate cancer rates differ significantly among racial and ethnic groups. African American men have an incidence of prostate cancer about 150/100,000 person years. Caucasian men have an incidence at about 100/100,000 person-years, and Asian men have an incidence of about 30 to 40/100,000 person-years.
Family history is an important factor in determining whether a man is at an increased risk for prostate cancer. The more family members and the earlier the age of onset of cancer in related family members increase the risk.
JN: If among men whose fathers had prostate cancer 55% of them also developed prostate cancer, is it scientifically reasonable to conclude that a principal factor in the case of the sons who developed cancer was genetic? If so, do we have any studies that suggest why 45% of the sons who didn’t develop prostate cancer escaped the disease?
KL: We do not entirely understand the genetic influence of prostate cancer and its specific influence in individual cancer.
JN: What about gene therapy for prostate cancer?
KL: Gene therapy is receiving much attention as a potential treatment for many cancers. Currently, gene therapy is still an experimental strategy for prostate cancer treatment.
Term:
Gene therapy – a technique used to correct defective genes

{kind=link}