Diagnosing and treating pre-eclampsia
Does a doctor deciding that you have pre-eclampsia depend only on high BP measurements or will I have to undergo other tests as well?
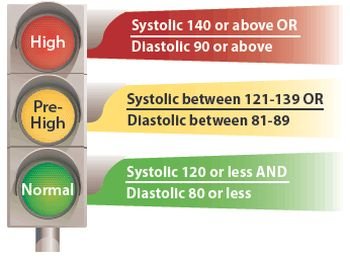
Your BP readings are important but yes, they do take other evidence into account. Pre-eclampsia will be suspected if your BP is 140/90 mmHg or more and is known to have been less than this before your pregnancy began, and/or if there is protein in your urine, and/or if you have some swelling of your whole body from increased fluid (oedema). Although most pregnant women will have some mild oedema (usually affecting their ankles and legs), protein in your urine and more severe oedema indicate that raised BP has caused some kidney damage. These are the earliest changes in the sequence of events that may, untreated, end with eclampsia. Occasionally pre-eclampsia is suspected for the first time because of poor growth of the baby when the midwife or doctor examines your abdomen. Babies in this circumstance are usually very quiet with the mother reporting a marked fall-off in the fetal movements.
You are considered to have mild pre-eclampsia if your diastolic pressure is between 90 and 99 mmHg, moderate if it is in the range 100–109 mmHg, and severe if it is 110 mmHg or more. If you have significant amounts of protein in your urine (most accurately measured on a 24-hour collection of urine), then pre-eclampsia is considered to be severe whatever the level of your BP. Blood tests may help in determining whether pre-clampsia has led to disturbance in your liver and kidneys or alteration in your ability to form clots.
Protein was found in my urine at my last visit. Does protein in the urine always mean that a woman has pre-eclampsia?
No. A bladder or kidney infection can also cause protein to appear in your urine, so the urine sample you provide should also be checked for infection. The urine tested needs to be a ‘clean catch’ or ‘midstream’ specimen, otherwise the germs thatnormally live in the vagina may be washed into the collecting tube and cause the sensitive urine testing strips (dipsticks) to give a false positive result. You provide a midstream (MSU) specimen by passing a little urine first before you collect your sample in the container provided. Sometimes you may be asked to collect all the urine you pass in 24 hours, to measure the total protein lost in your urine throughout the day. This should be less than 300 mg in 24 hours. Some people lose protein from their kidneys from time to time, without this signifying any damage.
Why does pre-eclampsia cause protein to collect in the urine?
Urine normally contains only water with a large variety of rather simple waste products (mainly urea and salt) dissolved in it. Proteins (which are large and complex chemical molecules) are normally filtered out and retained by your kidneys, and so do not appear in your urine. When BP rises for the first time in pregnancy, it rises much faster than ‘ordinary’ high BP in people who are not pregnant. Even though the actual level of raised BP may not be very high, because it has happened quickly, your kidneys have had less time to adapt to the new higher level and so are more easily damaged. The effect of even minor damage is that your kidneys begin to leak protein into your urine.
The amount of protein in your urine is roughly proportional to the severity of the damage to your kidneys. Your kidneys will recover to the pre-pregnancy state following pregnancy; however, occasionally, women are identified for the first time in pregnancy with pre-existing kidney damage. This will only become apparent if the kidneys have not returned to normal by 6 weeks following delivery.
If I already had high BP before my pregnancy, how can doctors recognize if I develop pre-eclampsia?
Blood pressure normally falls during pregnancy even in a woman whoalready high BP before she became pregnant (like you). Whatever your starting point, a rise above your pre-pregnancy BP level would be a cause for concern, and would alert your doctor or midwife to the possibility of pre-eclampsia. For those women for whom good pre-pregnancy BP measurements are not available, then BP measurements taken later in pregnancy can be compared with the readings taken early in pregnancy. Some research suggests that a diastolic pressure rising by more than 15 mmHg or a systolic pressure rising by more than 30 mmHg indicate a cause for concern. Urine tests, blood tests, and presence of oedema provide valuable additional information in these circumstances.
My legs became very swollen the last time I was pregnant, so my doctor was a bit concerned about pre-eclampsia, but stopped worrying when my BP and urine tests turned out to be OK. Please can you explain what was happening?
In severe pre-eclampsia, so much protein may be lost in the urine that the level of protein in blood falls. The blood cannot then retain all the water it contains; some leaks through the walls of the capillaries (the smallest blood vessels) to other parts of your body, making them swell. Because water tends to fall to the lowest point, this swelling first becomes obvious in your legs.
However, swollen legs are extremely common in pregnancy, and usually have nothing to do with pre-eclampsia. Anything that obstructs the flow of blood up your leg veins can cause raised BP in your veins (not your arteries, and arterial BP is what we are concerned with in pre-eclampsia). Fluid can then leak out of the veins into the skin, causing the same signs of oedema. The most obvious cause of such obstruction is the pregnant uterus (womb), and in late pregnancy some degree of oedema is almost inevitable in almost every pregnant woman. It can happen earlier in pregnancy in women who are overweight, or wear tight clothing, or stand for hours on end.
All these common causes of swollen legs can be distinguished from pre-eclampsia because they are not accompanied by protein in the urine. Finally, don’t forget that if only one leg swells, or one leg swells more than the other, the cause may be a deep vein blocked by a clot, a common and important complication of late pregnancy, which may need urgent treatment. See your doctor or midwife if you think this is happening.
If I do develop pre-eclampsia, is there a way for my doctors to treat it or even cure it?
There is no cure for pre-eclampsia other than delivery. Your obstetrician will need to consider the risks to you and your baby in determining the best timing and method of delivery. In late pregnancy it can be treated by starting labour early (induction) or by a planned or emergency caesarean section (an operation to deliver the baby through the abdomen) before labour starts. Although severe, rapidly progressing pre-eclampsia can occasionally begin at 24–26 weeks into the pregnancy, but this is very uncommon. Most women who get it develop a mild form of the disease at 34–36 weeks with small amounts of protein in the urine, and diastolic BP (the second of the two BP figures) in the 90-100 mmHg range. They usually do well if labour is induced a little early and deliver good sized babies, who can stay with their mothers on the ward. Babies who are very immature may need special care in a neonatal intensive care unit. Depending on how far you are on in your pregnancy, or whether this is your first or a later pregnancy, labour may be induced either by breaking your waters (called artificial rupture of membranes, or ARM) or by using prostaglandin (PG) pessaries or gel inserted into the vagina. Synthetic oxytocin (Syntocinon) may be used to make the uterus contract if labour does not start after the ARM or PG pessary. This has to be given by a drip into one of your veins. Sometimes this may be given immediately the ARM has been done. If your obstetrician decides that your pre-eclampsia needs drug treatment, then the most likely BP-lowering drugs to be used are either methyldopa, beta-blockers or a calcium-channel blocker (nifedipine). If these drugs are ineffective, then most obstetricians would use hydralazine (a vasodilator drug) orlabetalol (a beta-blocker by infusion – injection into a vein).
We used to be told that rest in bed was the most important treatment for pre-eclampsia, but obstetricians and midwives today don’t seem so concerned about this. Can you explain this?
Research studies have compared pregnant women with preeclampsia treated by traditional bed rest in hospital with similar women who simply took things easy at home – they have shown no difference at all in how well women (and their babies) got on.
Physical and mental rest is important, but many women get more rest if they are allowed up and about in their own homes than if they are compelled to lie in a hospital bed. However, women with pre-eclampsia who are being treated at home do need careful supervision, and should have their BP measured and their urine tested for protein at least once a day, and should be admitted to hospital immediately if they get abdominal pains or headaches.


{kind=link}