How to Treat Migraine. Home Remedies for Migraine
Preventative treatment
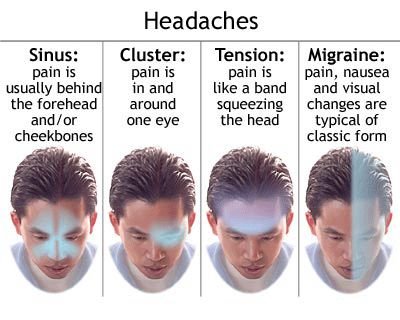
There are lots of different headaches and there are lots of different ways of treating them. The important thing is to find the right treatment for the right headache. This is true of preventative treatments as much as it is true of acute treatments.
Choosing when to use preventative drug treatment will vary from person to person, and deciding which drug can depend on a host of different factors.Remember that you don’t have to take any preventative drug for ever; just for long enough to break the cycle of frequent headache days. This can vary and may be for as little as three months or as long as six to twelve months; only you can decide what works for you. You often have little to lose and much, potentially, to gain by trying preventative medication.
PREVENTATIVE DRUG TREATMENT FOR MIGRAINE
My doctor has said that I need prophylaxis but I am not sure what it means. What is it?
Prophylaxis means ‘prevention’ and is used here to describe a drug taken on a daily basis to try to reduce the total number of headache days you are experiencing. In some people the attacks themselves can also become easier to treat.
If I take prophylaxis, will it stop all my migraines?
If you find the right drug and take it for long enough at the right dose, it can reduce the number of attacks you experience by at least 50%. It is unlikely to stop all of your attacks, though. The goal will be to reduce the total number of headache days you experience. You will still need an effective acute treatment for any breakthrough attacks that you may get. Remember: it will only stop some of the attacks some of the time.
Is preventative treatment any different from prophylaxis?
Preventative drug treatment and prophylaxis are just different words for the same thing. But preventing migraine is not just about taking tablets – it’s also thinking about the other things that you can do to raise your migraine threshold so that you are less likely to trigger a migraine. These include looking at your diet and your lifestyle to see if any changes would help you.
If I opt for prophylaxis, do I have to take it every day?
Prophylaxis will work only if you take it at the prescribed dose every day. This may seem tedious but it is the only way to get the best effect from whichever drug you choose. You also need to be sure to take it for long enough and reach a high enough dose to have the desired effect.
How do I know what dose I need to take in order for a preventative drug to work?
You – and your doctor – won’t know the right dose until you find it! Different drugs work differently in different people and at different doses. It is usually worth starting at the lowest dose, taking it for three months, and then increasing the dose if you have not noticed any reduction in headache days. ‘Start low and build slowly’ is a useful motto to follow to minimize side effects and allow you to find the right dose to reduce the number of headache days you have. If the first drug doesn’t work, it is always worth trying a different drug in the same class, or try a different type of drug altogether.
If I take preventative drugs, how long do I have to take them?
You need to take them long enough to have an effect. This usually means taking a particular dose for three months before deciding whether that dose is making a difference. Having found a drug, and a dose, that does reduce the number of headache days you experience, it is not easy to decide the right time to stop them. Usually six months is enough to break the cycle and reduce the number of times an attack starts.
If the headaches do recur, you could restart the medication or, if you have been slowly reducing the drugs, go back up to the dose that controlled your symptoms.
If prophylaxis works, how long can I take it for?
There is no benefit in taking it for ever. Six months is usually enough to break the cycle, once you have reached an effective dose. The reason for taking prophylaxis is to raise and then reset your migraine threshold. Deciding when to stop is about thinking where your threshold is and being aware of all the factors in your life that might push it down. If there are too many things around that push your threshold down, you might delay stopping your prophylaxis until things are a little more under control.
I have started on amitriptyline and been advised to increase the dose each week. Why so slowly – surely the quicker I get to the right dose the quicker I will notice an effect?
The main reason for increasing the dose slowly is to try to reduce the chance of side effects being a problem for you. It is one way of finding a dose that you can tolerate while reducing the number of headache days you have. Dose changes tend to be in small steps. The smallest step you can take with amitriptyline is 10 mg. The initial target dose is 30 mg daily; the next would be 50 mg. The maximum dose for amitriptyline is 150 mg in a day but this is rarely needed.
My friend has tried loads of different drugs but they all cause side effects with her. Is there any hope for me?
Everyone is different so there is no reason why you won’t be able to find a preventative drug that works and does not cause unacceptable side effects. Any drug has the ability to produce side effects and the symptoms do vary from drug to drug. Most people are able to take a drug and experience no difficulties at all. Some people are more sensitive to drugs and become aware of side effects.
Side effects can vary according to the particular drug, the dose used, how often you take the drug, and how quickly you build up the dose. Some side effects are more problematic than others and you will have to consider whether the benefits outweigh the disadvantages. Only you can decide but if you don’t try you will never know!
My sister has found that every time she stops her preventative drug her migraines start again after three to four weeks. Why is this?
It is not really possible to say exactly why. Preventative drugs cannot stop migraines happening forever – a migraine can happen at any time. A preventative drug breaks the cycle when the number of migraines you get increases and they don’t seem to want to settle down.
The frequency of your sister’s migraines depends on a lot of factors, and thinking about where her migraine threshold is may provide the answer to why the migraines start up again with the same sort of frequency.
I have tried several different drugs to stop my migraines but none of them seems to work. Why is that?
There may be many different reasons why they don’t seem to have worked. A major factor is that different people respond differently to drugs. You need to find the right dose of the right drug and you need to use it long enough for it to work. There are times when you need to do other things to push up your threshold so that the preventative drug gets a chance to work. Everyone is different and it may be that you haven’t found the right drug yet or the right dose. So keep trying. I have been given propranolol to help my migraine.
The nurse at the clinic says I’ll have to take it for three months before I’ll be able to tell if it is helping. Why so long?
You might notice some improvement within the first week or two but some people take longer to respond. (Some people stop the drug too early because it doesn’t seem to be working.) Taking the propranolol for three months at the lowest dose gives the drug a chance to have an effect at the lowest dose that will work. There is no point in taking a drug at too high a dose, as higher doses are more likely to cause side effects.
I have been talking to different people I’ve met at the clinic. One of them says that she took propranolol 80 mg and another said that he needed 240 mg. Why did it take such different doses to bring their migraines under control?
Essentially, everyone is different in how they respond to drugs. Propranolol works best if you have migraine and do not get any other headaches. It is easier to remember to take a tablet every day if you only have to take it once a day. Propranolol can be taken just once a day because it is available as a slow-release preparation. The first dose routinely prescribed is 80 mg; this can be stepped up to 160 mg and then to 240 mg, and occasionally to 320 mg. Each dose is taken once a day for three months, and the dose is increased only if there has been no significant or acceptable reduction in headache days.
Every drug I have tried has resulted in my putting on weight. Are there any drugs that won’t cause me to gain weight?
A lot of drugs can cause weight gain as a side effect, but not everyone necessarily experiences it as a problem. You have been quite unlucky to have had problems with all the drugs you’ve tried. The only drug used for migraine prevention that causes weight loss as a side effect is a drug newly licensed for use and its called topiramate.
I have been looking on the internet and have read that there are beta-blockers other than propranolol to help migraine. Is it worth giving them a go?
Yes, it is. Beta-blockers are a group or ‘classes of drugs that are usually used to treat high blood pressure or ease anxiety symptoms as well as reduce the frequency of migraine attacks. They are all slightly different in how well they do this, although the effect they have is viewed as a ‘class effect’. Some are seen as more likely to be of benefit than others on the basis of published research. Alternatives to propranolol include atenolol and metoprolol.
I have asthma so can’t take beta-blockers, which worked for my mum. What else can I take?
Unfortunately, beta-blockers and asthma do not mix. If you want to try a preventative drug, you could try an anti-epilepsy drug or a tricyclic antidepressant.
If you want to avoid taking any preventative drugs, you might want to focus on diet and lifestyle changes. Why has my doctor given me an epilepsy drug to stop my migraines?
Anti-epilepsy drugs (AEDs) are used to treat chronic pain and migraine as well as epilepsy. Crudely speaking, the anti-epilepsy drug is stabilizing the brain and preventing it from causing the symptom. That symptom might be an epileptic fit, feeling pain or a migraine attack.
My doctor said he was prescribing me Epilim but the box says sodium valproate; is it the same thing?
It was Epilim that the specialist nurse suggested and I don’t want to be given the wrong drug. Epilim is the brand name of sodium valproate, so they are the same and you have the right drug. In general terms the ‘names’ are interchangeable. Most drugs these days are prescribed by their generic name but there are some exceptions when it is crucial to get exactly the right amount of drug in the bloodstream and Epilim is one of them. Epilim is ideally to be taken twice a day as a slow-release preparation (Epilim Chrono). Using the brand name means that you know exactly how quickly, or slowly, the drug is released, so you know exactly how much drug is getting into the system, where it needs to be.
I was given a drug called Epilim that worked really well but my hair started falling out. My doctor said that I would have to stop taking the drug but I am not keen as it has stopped my migraines. What are my options?
Hair loss is one of the side effects that Epilim (sodium valproate) can cause. Epilim is a drug used to treat epilepsy, and trying a different anti-epilepsy drug (AED) might give you the same benefit without this particular side effect. If you don’t want to try a different AED, you might consider a beta-blocker or a tricyclic antidepressant.
Of course, any of the alternatives can lead to side effects, but they will be different from those found with Epilim. My sister put loads of weight on when she took Epilim. Will the same happen to me?
The simple answer to that is: not necessarily. One of the recognized side effects is weight gain but it doesn’t happen to everybody. It is certainly worth trying but if you find that you do start to gain weight, stop it and try something different. I am getting confused by all the different tablets my daughter has been given. She has been taking Epilim (sodium valproate) and some of the tablets are 200 mg and some are 300 mg, and they have ‘Chrono’ on the box.
Why does she have different strength tablets? Or are they all the same?
Chrono’ is the bit of the name that tells you that it is a slow-release tablet. This means that you take the tablet twice a day. There are three Epilim Chrono tablets – 200 mg, 300 mg and 500 mg – so they are the same drug but they are different strengths.
I expect that your daughter was given the 200 mg tablets to start with, to see if she would get any side effects from the drug. It is usual to take this dose for three or four days before increasing it, perhaps to 300 mg as the next step. I usually do what I refer to as a ‘slow up-titration’ – increasing the dose in the smallest possible steps – to try to minimize any side effects that might be experienced.
My specialist nurse has told me that I need to have regular blood tests when I start taking Epilim. Why is that?
Many drugs are processed by the liver, to break them down and inactivate them. In some people, the enzymes in their liver can be affected by these drugs and become overactive. In order to ensure that your liver is not being adversely affected, regular blood tests over the first few weeks and months is the only way to confirm this. If there is little or no change, it is safe to carry on taking the Epilim.
I have been taking Epilim for six months and have found that my migraines got better initially, but they’ve become more frequent again over the last few weeks. Is there a maximum dose I can take?
The usual maximum dose for Epilim is 2g a day, usually in two separate doses. There is no right or wrong dose, and it is often worth going up to the maximum dose of 1g twice daily to see what works for you.
I have tried a couple of AEDs but they either did not work or caused side effects that I found unpleasant. Are there any other AEDs that work for migraine?
There are several different AEDs used for migraine prophylaxis. Epilim (sodium valproate) is one; others include topiramate, gabapentin and levetiracetam. Topiramate has recently been licensed for use in migraine prevention and is certainly worth trying. It may be that your doctor will be happy to prescribe it, even though the current license advice is that it should be from a hospital specialist.
My friend has used topiramate for her migraine and it worked really well. Could I try it?
Yes, you could. Topiramate works well in preventing migraine but some people experience a lot of side effects. You will only find out how well it works for you if you try it, and the same applies to side effects.
The specialist nurse has suggested I use topiramate for migraine. What sort of side effects can I expect?
There are many different side effects that you might experience but the commonest tend to be paraesthesia (e.g. ‘pins and needles’ or prickling sensation) and sleep disturbance. In some people there are mood changes and emotional disturbances including anxiety, nervousness, and depression. The most notable side effect is that it can cause weight loss; it is the only preventative migraine drug that has weight loss rather than weight gain listed as a side effect.
Some people experience few or no side effects; others who have mild side effects feel that the benefit is worth it. The only way to know is to try it.
It has been suggested that I try topiramate for my migraine. What sort of dose do I need to take?
The usual dose for migraine prevention is 50 mg twice a day. Some people notice a benefit below this dose, and others need to get up to this dose. I usually start people on the 15 mg capsules, increasing the dose by 15 mg every two weeks to minimise the development of side effects, and ideally stop at the lowest dose needed to produce an effect.
I have just started topiramate but have been getting some funny sensations affecting my hands and feet. Is that normal?
This is one of the recognized side effects of topiramate and in that sense is normal. Only you can decide if the benefit you are getting from your topiramate is worth the side effects you are experiencing.
I’ve tried Epilim (sodium valproate) and topiramate with limited benefit. I have been reading on the internet about gabapentin and levetiracetam. Can you tell me anything about them?
Gabapentin is an AED that is used in treating epilepsy and chronic pain problems, such as back and neck pain and even neuralgia. There is some evidence to suggest that it can help some people reduce the number of migraine attacks that they experience. There are a range of side effects that you may experience; they include nausea and vomiting, diarrhoea, dizziness, drowsiness, fatigue, paraesthesia as well as some mood and emotional changes.
Levetiracetam is used mainly in epilepsy but some studies suggest that it can help in reducing migraine frequency. More studies are planned so, if you have had little or no benefit from other drugs, it is worth trying levetiracetam. There are a range of side effects associated with levetiracetam; they include drowsiness and dizziness, less commonly nausea, diarrhoea, emotional changes and double vision.
My doctor has suggested I should take the antidepressant amitriptyline to stop my headache, but I am not depressed and don’t want to take it. Why has he suggested it?
Although amitriptyline was developed to treat depression, it has also been used successfully to treat chronic pain – and, of course, headache is a form of chronic pain. If you view taking the drug as a way of stabilizing the way your brain responds, it makes a little more sense! By raising your migraine threshold, it should reduce the chance of a migraine being triggered.
I have been taking amitriptyline but have found that if I take more than 20 mg I am too sleepy to get up in the morning. It seems to be easing my migraines, though, so is there anything I can do?
That rather depends on what time you actually take the amitriptyline. If you are having difficulty waking in the morning, try taking it 12 hours before you want to get up. If that doesn’t work, you could try a similar drug called imipramine, which may cause you few or no side effects.
I have been given amitriptyline for my migraines but my sister was given imipramine. Is it any better?
That is not an easy question to answer, as it rather depends on what you mean by ‘better’. If amitriptyline causes you to experience side effects, imipramine may suit you better. If the amitriptyline does not reduce the number of headache days you get, imipramine might suit you better. ‘Better’ is really what works for you.
Why do antidepressants and epilepsy drugs work in migraine when they were designed for such different problems in the first place?
I am not sure that anyone can really answer that question. Both types or ‘classes’ of drug are designed to have an effect on the brain, and both migraine and epilepsy are conditions that are caused by brain changes. Anything that can stabilize the brain’s response and prevent these changes from occurring will prevent events happening, be they an epileptic or a migraine attack.
I am a little curious as my specialist nurse says that antidepressants will help my migraines but amitriptyline and similar drugs have always made me feel really drowsy. Is there any other sort of antidepressant that I can take that has fewer side effects?
Amitriptyline is one of the tricyclic antidepressants (TCAD) group or class of drugs. Imipramine, dosulepin and nortriptyline are all TCADs. Different people react differently to different drugs, and it may be that with others you will not feel as drowsy as with one of the ones you have tried already.
There is another type of antidepressant, collectively referred to as selective serotonin re-uptake inhibitors (SSRIs), that is not associated with the same sort of side effects as TCADs but there is no good evidence that these drugs are helpful in the management of migraine.

{kind=link}