If You Could See What I See – Body Dysmorphic Disorder (Body Image) (Video)
Body Dysmorphic Disorder (BDD)
What is Body Dysmorphic Disorder?
Body Dysmorphic Disorder (BDD) is perhaps the most severe form of body image disturbance. It is described in the DSM-IV-TR as a preoccupation with some imagined defect in physical appearance or an excessive concern with a minor physical irregularity. For example, a person may have severe distress over one or more areas of their body: a facial feature, skin blemish, or body hair; or maybe their head, thighs, stomach, breast, or buttocks. Common complaints associated with BDD involve real or imagined acne, wrinkles, thinning hair, scars, swelling, or facial asymmetry. Also common are concerns with the shape or size of a body part such as the nose, eyes, ears, mouth, jaw, chin, cheeks, or head. In BDD, the preoccupation with a perceived flaw is excessive and causes significant distress or impairment in functioning.
Most people with BDD find their preoccupations difficult to control, to the point that thoughts about their “defect” come to dominate their lives. In order to cope with their distress, many with BDD will continually ask for reassurance from others about their perceived flaw. Some people engage in excessive grooming behaviors and self-scrutiny (e.g., checking themselves frequently with a mirror or magnifying glass) in an attempt to temporarily decrease anxiety about their perceived flaw; however, this generally leads to further preoccupation and distress. Others avoid mirrors altogether out of low self-esteem, shame, embarrassment, or fear of rejection. BDD may lead to social isolation, work problems, and avoidance of social interactions. In extreme cases, individuals may only leave their house at night or become housebound altogether. Some with BDD will attempt to correct their “defect” through cosmetic surgeries; however, these procedures may actually cause the disorder to worsen and lead to an even greater preoccupation with appearance. The distress associated with BDD can lead to hospitalization, suicidal thoughts, and suicide.
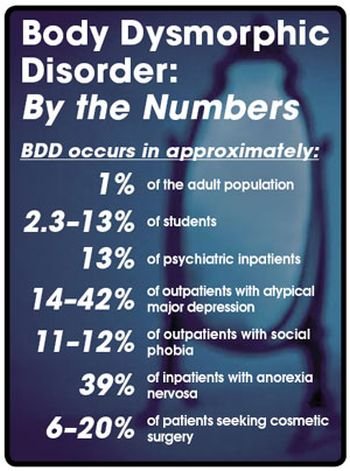
BDD affects up to 2% of the U.S. population, affecting both males and females in equal numbers. Symptoms of the disorder usually begin in adolescence or childhood (70% of cases begin before age 18); however, the condition may go undiagnosed for years, perhaps because individuals experiencing symptoms associated with BDD are reluctant to express their concerns with others. Many BDD patients have a co-occurring condition, such as depression, anxiety, or obsessive-compulsive disorder.
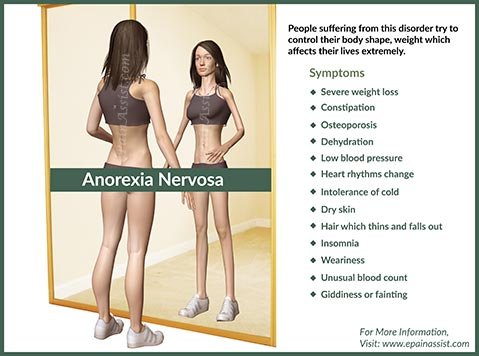
As noted in Eating Disorders and Obesity: A Comprehensive Handbook, Second Edition, BDD and eating disorders have some obvious similarities, such as a preoccupation with perceived flaws of appearance, a disturbance in body image, and a sense that one’s body is unacceptable. However, for patients with BDD, the focus tends to be more on specific body parts than on body shape or weight. According to the DSM-IV-TR, a person can receive both a diagnosis of BDD and anorexia if warranted, but a person is not diagnosed with BDD if their preoccupation and distress is only restricted to “fatness.” This person’s diagnosis would focus solely on the appropriate eating disorder.
BDD is generally considered a chronic condition with a high rate of relapse. Research on this disorder is in its infancy, although two treatment methods have been identified as being helpful: cognitive-behavioral therapy and certain psychiatric medications. Both have been shown to decrease the symptoms and distress associated with BDD.
How does a healthcare professional assess for and treat body image disturbance?
Assessment can be accomplished through patient interview, combined with the use of various professional assessment materials. In a clinical interview, one’s healthcare professional may inquire about a patient’s weight history (i.e., current, highest, lowest, longest standing body weight) and subjective satisfaction with weight and body image. The interview may also screen for a history of teasing about appearance and weight, family history of eating disorders, body image dissatisfaction, patient eating disorder behavior, body checking behavior, and other issues salient to body image. Self-report questionnaires are often used to assess body image disturbance and dissatisfaction.
Additional self-report questionnaires can be found in The Body Image Workbook by Thomas Cash.
In addition, scientific research has yielded a number of useful measures that utilize figure drawings to assess for body image disturbance. These measures involve viewing a series of artist sketches featuring male or female figures. Participants are then asked to respond to questions that pertain to their perception of the figures. An example of this type of measure is the Bidimensional Body Evaluation Scale for Women (BBESW) and consists of 32 figures that vary in body fatness and muscularity. Patients are shown the figure array, which is printed on an 8½ × 11 sheet of paper, and are asked to respond to the following questions:
1. Which figure do you think you look like most of the time?
2. Which figure would you most like to look like, in an ideal world?
3. Which figure do you think the social environment (society, friends, TV, magazines, movies, etc.) wants you to look like?
4. Which figure do you think men find most attractive?
5. Which figure do you think women find most attractive?
Various therapeutic techniques have shown promise for improving body image perception. Some are experiential in nature. For example, in order to help patients understand the phenomenon of body image distortion, some therapists will ask them to draw an outline of how they think their body looks on a large piece of butcher paper. The therapist will then tape the paper up on a wall and literally trace the outline of their patient’s body shape on the paper while he or she stands against it. The patient is then asked to turn around and view the difference between their perceived body image, as he or she drew it, and their actual body size. Other therapeutic techniques include guided imagery, talk therapy, behavioral interventions, and self-help manuals; each has yielded some measure of success.
A treatment approach increasing in popularity is cognitive behavioral therapy (CBT). According to psychologist Thomas Cash, CBT treatment of body image issues has been shown to result in increased body satisfaction, decreased investment in appearance, reduced body image distress, and an improvement in the areas of self-esteem, social functioning, and eating behaviors. Cognitive-behavioral therapy includes a psycho education component that helps patients understand how altering one’s thoughts about body image and appearance can lead to decreased body image disturbance and a healthier
approach to body shape, appearance, and weight. Cognitive behavioral therapy utilizes a variety of exercises, including relaxation techniques, journaling, behavior modification, and “homework” exercises aimed at improving body image acceptance and modifying distorted personal beliefs about body image, shape, weight, and appearance.
What are some practical ways to improve body image?
There are a number of things a person can do at home to improve body image and reduce body dissatisfaction. However, depending on the person’s level of body image disturbance, professional support and treatment may be warranted. This is especially true if eating disorder symptoms are present. The following is a list of helpful suggestions for building a healthy, positive body image. Although one list cannot automatically tell you how to turn negative thoughts about body image into positive ones, it can be a step toward appreciating, respecting, and valuing yourself and the body that you have been given:
- Recognize that bodies come in all different shapes and sizes. There is no one “right” body size. Your body is not, and should not be, like anyone else’s.
- Appreciate all that your body can do. Honor it. Respect it. Fuel it.
- Focus. Create a list of all the things your body lets you do. Read it and add to it often. Remember that your body is the instrument of your life, not just an ornament.
- Socialize. Don’t let your weight or shape keep you from activities that you enjoy.
- Count your blessings, not your blemishes.
- Be your body’s friend and supporter, not its enemy. Care for it.
- Express gratitude. Every morning when you wake up, thank your body for resting and rejuvenating itself so you can enjoy the day. Every evening when you go to bed, tell your body how much you appreciate what it has allowed you to do throughout the day.
- Keep a list of positive things about yourself-without mentioning your appearance. Add to it, and read it often. Choose to find beauty in the world and in yourself.
- Consider getting rid of the scale. It’s what’s inside that count.
- Remember that your size, shape, and weight do not determine your worth as a person. You are not just your body.
- Become a critical viewer of the media. Begin to question whether the sculpted images of men and waiflike images of women are realistic. Pay attention to images, slogans, or attitudes that make you feel bad about yourself or your body. Protest these messages: Write a letter to the advertiser or talk back to the image or message.
- Think about all of the things you could accomplish for others with the time and energy you spend worrying about your body and appearance. Try one! Reaching out to help another person can be a great way to make a positive change in our world and to feel better about you!
- Surround yourself with positive people who care about your well-being. Find friends who are not overly concerned with body weight and appearance.
- Talk. When you are feeling badly, talk about it!



{kind=link}