VIDEO
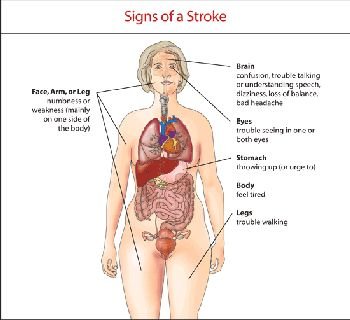
Symptoms of a Stroke : How to Identify a Stroke
(Doctor only)
Ischemic stroke prevention: general measures
Educate your patients so they can take an active role in their health care and secondary prevention of ischemic stroke.
Try to convert patients to the medications that they will be going home on prior to discharge, to make sure they tolerate them. Also, take cost issues into account. A patient who cannot afford the medications will not take them.
The following are derived from the most recently published guidelines, which should be consulted for details.
(1) Control Risk Factors
. Hypertension (based on SHEP trial, and others).
– ACE inhibitors (HOPE, PROGRESS trials).
– Diuretics and calcium channel blockers (ALLHAT trial).
Elevated lipids:
– Statins (several trials, including MRC Heart Protection Study).
– Target LDL <70 mg/dl according to the most recent guidelines for high-risk cardiovascular patients.
– Be sure to get baseline liver functions before starting statin therapy.
. Smoking:
-Cessation counseling and pharmacotherapy.
. Diabetes:
– Identification.
– Treatment, including diet.
Hyperhomocysteinemia:
– May justify folic acid, B12, B6 treatment, but so far there is no evidence that vitamins – including folic acid – are effective for stroke prevention in general (VISP study).
– Therefore, since there is no effective treatment for this risk factor for stroke, routine screening for hyperhomocysteinemia is probably not cost-effective.
. Estrogen use (WEST trial, Women’s Health Initiative):
– Avoid in most cases.
. Drugs of abuse and alcohol:
– Should be avoided and discouraged, especially vasoactive drugs such as cocaine and amphetamines.
No more than two drinks per day.
(2) Antithrombotic or Anticoagulant Medications
. Aspirin (many studies).<0% relative risk reduction of secondary stroke/other vascular events. Doses of 50mg daily or higher; usually give 81 or 325 mg.
. Aspirin/dipyridamole ER (Aggrenox, Asasantin). ESPS-1 and ESPS-2 trials; 30% better than aspirin alone.
– The PRoFESS trial (ongoing) is comparing aspirin/dipyridamole ER (Aggrenox) to clopidogrel (Plavix).
. Clopidogrel (Plavix).
– CAPRIE trial. Slightly better than aspirin, particularly in patients with peripheral vascular disease, and better tolerated.
. Aspirin/clopidogrel combination.
Long-term use increases bleeding rate without benefit of greater stroke prevention (MATCH and CHARISMA studies).
Therefore the combination is not recommended long-term (more than a few days) unless the patient has had a recent stent placed.
. Warfarin (Coumadin). For most of the following, the use of warfarin can be considered based on either randomized trials (level A) or consensus recommendations (level C). However, except for those with Class 1 evidence (i.e., where there is general agreement with its use), either antiplatelet drugs or warfarin can be used.
– Atrial fibrillation except for ‘‘lone AF’’ (see below) (SPAF trials). Class 1, level A evidence.
– Critical extracranial carotid stenosis. String sign or occlusion (anecdotal experience).
– Basilar thrombosis/stenosis (anecdotal experience).
– Arterial dissection (consensus statements).
– Other ‘‘embologenic’’ cardiac conditions:
. Rheumatic valvular disease or mechanical valve (class 1 evidence)
. Low left ventricular ejection fraction (<30%) (consensus statements)
. Akinesis or severe hypokinesis of left ventricle segments (especially anterior wall or apex) (consensus statements)
. Stroke soon after myocardial infarction, especially if mural thrombus is identified on TTE (randomized studies)
. Aortic atheroma >4mm (from SPAF III subgroup analysis, consensus recommendation)
– Embolic-looking cryptogenic stroke (randomized trial – WARSS subgroup analysis)
– Stroke patients with documented coagulopathy (consensus statements)
. Especially if history or evidence of venous thrombosis, or pulmonary embolism
. Also patients with full antiphospholipid antibody syndrome (venous thrombosis, miscarriages, livedo reticularis)
– Venous infarction due to cerebral venous sinus thrombosis (consensus statements)
. Based on the following randomized trials, warfarin is not routinely indicated for:
– Stroke due to intracranial atherosclerosis (WASID study),
– Most non-cardioembolic strokes (WARSS),
– Most stroke patients with positive antiphospholipid antibody (APASS: a WARSS substudy), or
– Most patients with PFO (PICCS: a WARSS substudy).

{kind=link}