The Myth about Blood Sugars and Diabetes – Video
Diabetes UK – Care, Connect, Campaign
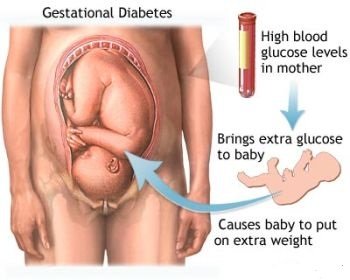
Centers for Disease Control and Prevention – USA GOVERNMENT – Diabetes and Pregnancy: Erin’s Story
Termination of pregnancy
I have become pregnant and really don’t want a baby at the moment. Are diabetes grounds for termination of pregnancy?
No, not unless your doctor considers that the pregnancy would be detrimental to your health, which may occasionally be the case. All the reasons for termination of pregnancy apply equally to people without diabetes as to people with diabetes.
I am going into hospital for an abortion. I am worried that the doctors might not do it as I have diabetes. Should I have told someone?
There is no added hazard for women with diabetes, who undergo termination of pregnancy, and care of the diabetes during this operation does not raise any special difficulties but it is still a good idea to tell your gynaecologist.
Infertility
I have recently got married and my wife and I are keen to start a family. Are people with diabetes more likely to be infertile than those who do not have diabetes?
There is nothing to suggest that men with diabetes are any less fertile than men who do not have diabetes and this is generally true also for women. In the case of women, however, extremely poor diabetes control with consistently high blood glucose readings is associated with reduced fertility. This is probably just as well as there is good evidence to show that the outcome of pregnancy is much worse in women who conceive when their control is poor. I have been trying for a baby for years and we have now decided to go for fertility counselling and possible treatment.
Can people with diabetes expect the same treatment for infertility as people without?
Yes. As mentioned in the previous question, diabetes is rarely the cause of infertility. If control is anything other than excellent, then improving control should be the first goal. If that is not successful than expert opinion on management from a specialist is the next step.
Pregnancy
Pregnancy was the first aspect of life with diabetes where it was shown without any doubt that poor blood glucose control was associated with many complications for both mother and child and that these complications were avoidable by strict control.
The outcome for women with diabetes who are pregnant and for the babies that they carry is directly related to how successful these mothers are in controlling their blood glucose concentration. If control is perfect from the moment of conception to delivery, then the risks of pregnancy to mother and baby are little greater than in women without diabetes.
We now know that poor control when the egg is fertilized (conception) can affect the way in which the egg divides and changesinto the fetus (in which all organs and limbs are present but very small) in such a way as to cause congenital abnormalities (such as harelip, absence of the bone at the base of the spine, and holes in the heart). The risk of this happening can be reduced to a minimum, and possibly even eliminated, by ensuring perfect control (normal HbA1c) before you become pregnant.
For women who become pregnant when their control is poor, there will be an increased risk of congenital abnormalities in their babies – some of which may be detectable by ultrasound very early in pregnancy, when termination is possible, if a major defect is found. When no defect is detected, the outcome of the pregnancy will still be dictated by the mother’s degree of control during her 40 weeks of pregnancy and during labour and delivery.
Modern antenatal care is usually shared between the diabetes specialist and the obstetrician, often at a joint clinic. So long as control remains perfect (normal HbA1c) and pregnancy progresses normally, there is no need for hospital admission. With the excellent control that is now possible, the baby will develop normally and we believe that the pregnancy can be allowed to go to its natural term (40 weeks). If spontaneous labour begins, the procedure is no different from that for a woman without diabetes, other than the continued need to keep the mother’s blood glucose normal to prevent hypoglycaemia in the infant shortly after birth.
Women with diabetes are not immune to obstetric and ante-natal complications and these will be treated in the same way as they would be in women without diabetes. If a woman cannot achieve satisfactory control of her diabetes at home, then her admission to hospital becomes essential, but there are very few mothers who cannot achieve and maintain normal blood glucose values as an outpatient, at least while they are pregnant. It is a remarkable example of the importance of motivation in the struggle for good diabetes control. The single-mindedness of a pregnant woman makes her able to cope with almost anything to protect her growing baby from harm. Sadly this motivation is often lost once the pregnancy is over and control slips back to where it was before.
A very comprehensive pregnancy magazine is available from Diabetes UK.
Prepregnancy
The man I am going to marry has diabetes. Will there be any risk of any children we have in having diabetes?
If you do not have diabetes yourself and there is no diabetes in your family, then the risk of your children developing diabetes in childhood or adolescence, if their father has diabetes, is probably about 1 in 20. Provided that you are both in good health it is certainly all right to have a family. If you and your fiancé both had Type 1 diabetes, then there would be an even greater risk of your children developing diabetes.
There is a rare form of Type 2 diabetes in which there is a strong hereditary tendency. This is called maturity onset diabetes of the young, commonly known as MODY. Were you or your fiancé to have this, the risk of your children getting diabetes of this unusual kind would then be rather high. It is often a relatively mild form of diabetes and runs true to type throughout the generations.
The study of inheritance of diabetes is a complicated subject and you would be well advised to discuss this further with your specialist or a professional genetic counsellor.
I am worried that, if I become pregnant whilst my husband’s diabetes is uncontrolled, the child will suffer – am I right?
No. There is no known way in which poor control of your husband’s diabetes can affect the development of your child.
I am 25 years old and have Type 1 diabetes. My husband and I plan to start a family but first I would like to complete a 3 year degree course at university. By the time this course finishes I will be 29. Can you tell me if I shall then be too old to have a baby?
You pose a difficult question as to the ideal age at which someone with diabetes should have a baby. The age of 29 is not too old tostart a family but there are certain advantages in starting younger, particularly if you have diabetes and if you plan more than one pregnancy. Starting a family may be hard work whether you have diabetes or not. If you add increasing age to the difficulties, we are sure that you will understand why it is normally recommended starting earlier rather than later. It is difficult to give exact personal advice to individual people and the right person to talk to is your clinic doctor who knows both you and your diabetes.
I have diabetes treated by tablets, which I chose to take rather than insulin, and I want to become pregnant again. As I have had a previous miscarriage, I am worried about the chance of this recurring. Both my husband and I smoke a lot. How can I make sure that this pregnancy is successful?
Your control of your diabetes will certainly affect the outcome of your pregnancy – better control leads to more successful pregnancies. As you are planning your pregnancy, you can make sure that you establish good control before conception. Your control is probably best maintained by either diet alone or, if this fails, by diet with insulin. We do not advise women to take tablets throughout pregnancy, although they do not harm the baby if they are taken inadvertently in the early part of pregnancy. The tablets can cross into the baby’s circulation and stimulate insulin secretion from the pancreas causing hypoglycaemia in the baby shortly after birth.
It should also be said here that most women of childbearing age are already being treated with insulin, so they are not normally faced with your decisions. You obviously know already that smoking affects the baby and that heavy smoking is associated with more miscarriages and smaller babies. In asking the question we suspect that you already know the answer – take insulin and give up smoking. There is also more recent evidence to link even modest regular alcohol intake in pregnancy with an unfavourable outcome as far as the baby is concerned, so we suggest that you should stop drinking alcohol until the pregnancy is over.
Why must I ensure that my diabetes control is perfect during pregnancy?
This is to ensure that you reduce the risks to yourself and your baby to an absolute minimum. If you are able to achieve this degree of control from before the time of conception through to the time of delivery, you can reduce the risks to your baby and these risks will be virtually indistinguishable from those to babies born to women without diabetes. On the other hand, if you do not control your diabetes properly and pay no attention to it, then the risk to your baby increases dramatically.


{kind=link}