3D Medical Animation – What is a Heart Attack? (Video)
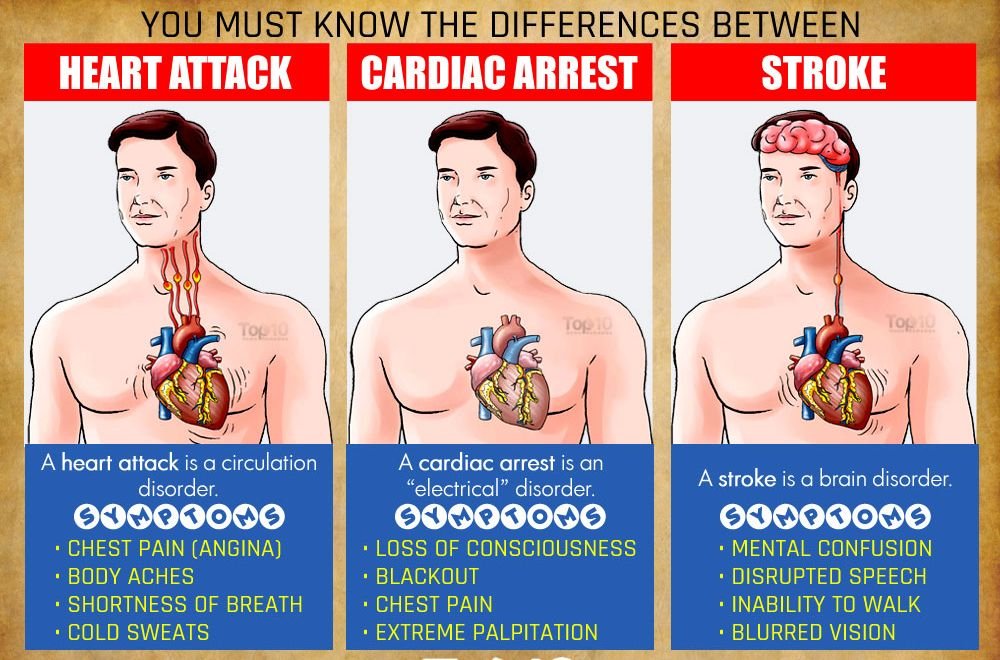
Signs of heart attack, cardiac arrest and sudden arrhythmia death syndrome (SADS)

What tests can detect and diagnose various arrhythmias?
Many tests can detect and diagnose arrhythmias. An electrocardiogram (ECG or EKG) is a recording of the electrical events of your heart through wires and electrodes that doctors attach to the skin of your arms, legs, and chest wall. The ECG device records electrical events by displaying wave forms on a monitor or printing them on paper. Routine ECG tracing records these electrical events for 12 seconds, allowing your doctor to detect and diagnose various arrhythmias. When a routine ECG does not detect a suspected or expected arrhythmia, however, other diagnostic tests may be necessary (discussed shortly).
On the ECG paper, the initial small and round wave, called the P wave, represents the electrical stimulation of the atria. The tallest wave after the P wave is the QRS complex, which represents the stimulation of the ventricles. Another relatively large, triangular wave is the T wave; it represents the period when the ventricles “recharge” their electrical forces to be ready for the next stimulation. These electrical events in total represent one heart cycle, and the normal heart rhythm continues in a healthy heart (called normal sinus rhythm). When something disturbs the normal heart rhythm, various arrhythmias will occur.
An ambulatory ECG (or Holter monitor ECG, named after the scientist who invented it) is a continuous recording of the electrical events of your heart for 24 hours (sometimes up to 48-72) hours). The Holter monitor is small (about the size of a small camera). It’s a portable ECG recorder, worn on a strap over your shoulder or around your waist. Several electrodes are attached to the skin on your chest, and they’re connected by wires to the ECG recorder. You would be instructed to record any signs or symptoms in a diary that would match any such activities.
The Holter monitor ECG records continuously on tape (or on computer chips). When you return the monitor to your doctor’s office or to the heart station of a hospital, a computer plays back and analyzes the tape and prints out the Holter monitor ECG diagnosis so a cardiologist can review it for a final diagnosis.
The event recorder is another form of ambulatory ECG. It’s similar to a Holter monitor ECG in that you would wear it for several days or weeks, but it’s not for continuous recording. When any symptom occurs or when you feel what you think is an arrhythmia, you push a button, and the ECG records for 1 to 2 minutes. The event recorder is most useful for occasional arrhythmias.
When any arrhythmia is considered to occur during physical exertion, a stress test (exercise ECG test) is very valuable. The most commonly used is a treadmill (monitor-driven) stress test. In a stress, or exercise ECG test, you walk on a treadmill (or ride a stationary bicycle) while a machine records an ECG of your heart’s electrical activity. The stress test can reveal any exercise-related arrhythmia that may not be found during a resting ECG.
As described earlier, a stress test is extremely valuable for the evaluation of chest pain, particularly angina, but a stress test should not be performed when an acute heart attack is in progress or is strongly suspected.
The tilt table test is a useful diagnostic tool to evaluate fainting spells (syncope) or near-syncope that may result from certain arrhythmias. In this test, you would lie on a table that can be moved to almost an upright position while a doctor continuously monitors your ECG, BP, and symptoms. Of course, the tilt table test should not be performed when an acute heart attack is in progress.
When the abovementioned tests fail to disclose the necessary diagnostic and therapeutic information, doctors may perform an electrophysiologic study (EPS) to assess the exact nature of a difficult problem. Thus, an EPS is usually recommended for those with life threatening arrhythmias, especially during or soon after an acute heart attack. The EPS is also used to detect and diagnose any suspected arrhythmias that are otherwise not detected.
During the EPS, a doctor inserts a special electrode catheter (a long, thin, flexible wire) into your veins and guides it into your heart. Using such catheters, doctors can identify the exact site causing a life-threatening arrhythmia. Thus, the EPS is very useful not only for the diagnosis of life-threatening arrhythmias but for proper management of a disorder.
Terms:
Ambulatory ECG – test noninvasive diagnostic test that records the electrical activity of the heart for 24 hours using a portable tape recorder to detect any abnormality of heart rhythm (also called a Holter monitor).
Event recorder – form of ambulatory ECG device that records only when an arrhythmia occurs.
Exercise ECG test – noninvasive diagnostic test for coronary artery disease using a motor-driven treadmill, bicycle, or certain chemicals. Also known as a stress test.
Tilt table test – useful diagnostic tool to evaluate fainting spells (syncope or near-syncope).
Electrophysiologic – study insertion of a special electrode catheter into the veins and from there into the heart to identify the exact site causing life-threatening arrhythmias.
What are premature beats?
Premature beats (contractions) are heartbeats that occur earlier than the underlying cardiac cycle and momentarily interrupt your heart rhythm. Premature beats may arise from the atria (then they’re called atrial premature beats) or from the ventricles (in which case they’re called ventricular premature beats). They’re the most common arrhythmias. Premature beats may occur in healthy people, but they occur more frequently in those with various heart diseases. It can be said that almost all adults experience premature beats from time to time. Some people don’t even know it, but most experience some unpleasant feelings, such as “skipped heartbeats” or “funny sensation in the chest.”
By and large, healthy people don’t need active treatment for occasional premature beats other than avoiding possible stimulants, such as caffeine. On the other hand, patients with active heart disease, particularly a heart attack, need active treatment when ventricular premature beats occur very frequently in certain patterns (e.g., multiformed, meaning a different pattern in each premature beat). Under these circumstances, frequent ventricular premature beats may be considered a potential warning sign for more serious arrhythmias, such as ventricular tachycardia or fibrillation.
Almost all adults experience premature beats from time to time.
What is atrial fibrillation?
Atrial fibrillation (AF) occurs when electrical impulses arise from multiple sites in the atria (upper chambers) in a chaotic and uncoordinated fashion. Thus, the atrial wall can’t squeeze the blood down to the ventricles. Only some of the rapid atrial impulses travel down to the ventricles because the atrial impulses must slow down in the AV node, which acts as a “relay station.” The resulting irregular and usually (although not always) rapid heart rhythm is typical of AF.
When AF occurs, like most people you would experience some uncomfortable feelings: fluttering or pounding in your chest, weakness, light-headedness, shortness of breath, and chest discomfort with actual chest pain. The major concern is the increased risk for developing a stroke in people with recurrent or longstanding AF. AF tends to produce blood clots within the heart because of ineffective atrial contraction. Such blood clots may cause a blockage of the arteries in the brain, and that can cause a stroke.
Various medications are available to restore normal heart rhythm or at least to control rapid heart rate brought on by AF. Some people require electrical shock treatment to terminate AF.
Anticoagulants (blood-thinning medications) are recommended for treating patients with recurrent or chronic AF to prevent a potential stroke.
Term:
Anticoagulants – medications that interfere with or prevent blood clot formation
{kind=link}