VIDEO
Atrial Fibrillation Symptoms & Treatments
(Doctors only)
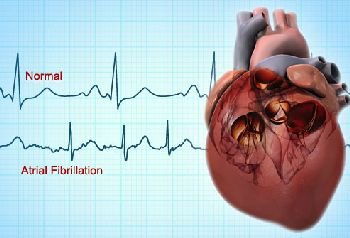
Atrial fibrillation (A fib)
A great deal is known about the prevention of stroke due to atrial fibrillation, and effective treatment is available.
In the Acute Stroke Setting
Acute stroke recurrence rate estimates vary.
From International Stroke Trial: 3.9% stroke recurrence rate in 14 days
Therefore, there is no reason to rush to anticoagulate with heparin or warfarin after an A-fib-related stroke.
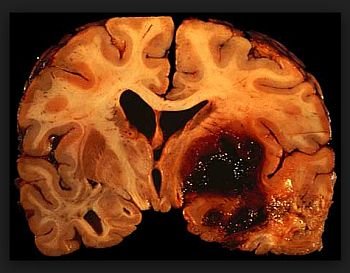
Wait 48-96 hours after a major stroke and repeat the CT (or MRI) first to exclude hemorrhagic transformation.
Natural History of Chronic Atrial Fibrillation
Valvular atrial fibrillation: stroke risk -17 x that of controls.
Non-valvular atrial fibrillation: stroke risk 6 x controls or – 5% per year.
Risk stratification:
Low risk: ‘‘lone’’ atrial fibrillation: age <60, none of the risk factors, and no history of TIA, stroke, or other embolic event: 0.5% stroke risk per year.
Moderate and high risk: variable combinations of age >75, decreased left ventricular function, hypertension, diabetes, and previous cardio embolism: up to 10%stroke risk per year.
Prior stroke/TIA/embolism: >10% stroke risk per year.
So, by definition, any atrial-fibrillation patient with embolic stroke or TIA is considered ‘‘high risk.’’
Age >80: >7% per year.
Echocardiograph risk features include: left ventricular dysfunction, left atrial enlargement or clot, mitral annular calcification, spontaneous echo contrast.
Treatment of Chronic Atrial Fibrillation
The choice of antiplatelet therapy vs. warfarin depends on the risk of stroke.
Primary stroke prevention with warfarin (Coumadin)
Ischemic stroke risk decreased to – 2% per year, or – 60% relative risk reduction.
Major bleeding risk: 1.5%–2% per year.
Increased risk with recent hemorrhage, falling, advanced age, alcohol binge, closed head injury, liver disease, aspirin, NSAIDs, cancer, age, previous stroke, uncontrolled hypertension.
ICH risk: 0.2–0.4% per year.
Age <75: 0.5% per year (data from SPAFII).
Age >75: 1.8% per year.
Target therapeutic INR is 2.0–3.0.
Primary stroke prevention with aspirin
Ischemic stroke risk decreased to – 4% per year, or 20% relative risk reduction.
Major bleeding risk: 0.3–0.9 % per year.
ICH risk: 0–0.3% per year.
Secondary Prevention
(Most of our cases on the stroke service)
Warfarin reduces the risk of recurrent ischemic stroke from 10–12% per year to 4% per year.
Target INR: 2.0–3.0.

{kind=link}