VIDEO
Invasive Breast Cancer with Lung Metastases – 5 years after the Issels

I have heard that breast cancer grows more slowly in older women and doesn’t need to be treated. Is that true?
Cancer is a disease of aging, and the incidence of breast cancer is increasing faster in older women than in younger women. Older adults with cancer often have other chronic health problems and may be taking multiple medications, both of which can affect their cancer treatment plan.
Misconceptions and prejudice often prevent older patients from getting the cancer treatment that they need. The biology of breast cancer is different in older women than younger women. As patients age, their breast tumors more frequently express hormone receptors (estrogen, progesterone), they have lower rates of tumor cell growth, and lower over expression of HER2 (human epidermal growth factor receptor 2).
Though these are usually thought of as favorable factors, most recent studies show no major age-related differences in breast cancer survival. In fact, older women with metastases often have more aggressive disease than their younger counterparts. Chronological age alone should not be the only factor used to determine how and when to use life-prolonging or palliative anti-cancer treatment. Despite advanced age, men and women who are relatively well often have a life expectancy that may exceed their life expectancy with breast cancer.
The average 70-year-old woman is likely to live another 16 years. A similar 85-year-old can expect to live an additional 6 years and remain functionally independent for most of that time. Even an unwell 75-year old probably will live five more years; long enough to experience symptoms and early death from metastatic breast cancer.
Since older women have estrogen or progesterone receptor positive breast cancer, hormonal therapy is often an excellent treatment option. Aromatase inhibitors (like anastrozole) work better and generally have fewer side effects than tamoxifen in postmenopausal women. On the other hand, they are associated with an increased risk of osteoporosis and related fractures. It is, therefore, important for oncologists to monitor the bone health of these women with bone density (DEXA) scans. The appropriate use of calcium and bisphosphonates is an important adjunct to the use of these agents. Elderly breast cancer patients are particularly susceptible to chemotherapy-induced anemia, neutropenia, mucositis, diarrhea, and dehydration.
Though the side effects of cancer treatment are never less burdensome in the elderly, they can be managed by oncologists; especially geriatric oncologists, who work in teams with others who specialize in the care of the elderly. With appropriate care, healthy older women do just as well with chemotherapy as younger women.
Terms:
Hormone receptor – A protein on the surface or inside a cell that connects to a certain hormone (estrogen or progesterone) and causes changes in the cell.
HER2 – overexpression An excess of a certain protein (HER2) on the surface of a cell that may be related to a high number of abnormal or defective cells.
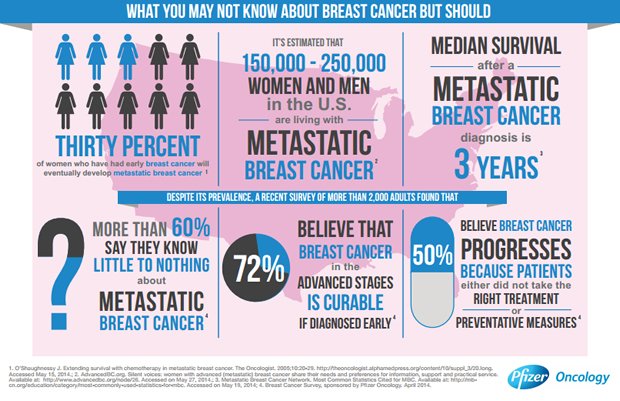
Metastases, metastasize – The spread of cancer from one part of the body to another.
Palliative care – Care to relieve the symptoms of cancer and to keep the best quality of life for as long as possible.
Estrogen/progesterone receptor positive cancer – Cancer that uses female hormones as a fuel to grow.
Aromatase inhibitor – Drugs that lower the amount of estrogen made in the body after menopause. This can slow or stop the growth of cancer that needs estrogen to grow.
Bone density (DEXA) scan – A test for osteoporosis and osteopenia.
Adjunct – A treatment that compliments another treatment.
Anemia – A condition in which the number of red blood cells is too low.
Neutropenia – An abnormally low number of a particular type of white blood cell called neutrophils.

{kind=link}