Ebola Virus Outbreak 2014 – WARNING
WHO: Ebola Outbreak Response in the Democratic Republic of the Congo
Who’s in Charge of Ebola at Hospitals? ‘Screaming That We’re Not Prepared’
Faces of the Ebola outbreak response – World Health Organization
Ebola virus disease – World Health Organization
Emerging virus infections
Emerging infections engender fear sometimes verging on panic as an unknown microbe appears without warning, infecting and killing populations, apparently indiscriminately. Although this scenario is more often the subject of horror movies than real life, the fact remains that today ‘new’ microbes are emerging with increasing frequency. Indeed, the first outbreak of SARS in 2003 and the swine flu pandemic in 2009 were very worrying until scientists discovered the cause and worked out control strategies.
The term ‘emerging virus infection’ refers to both the emergence of an infectious disease caused by a virus that is entirely new to the species it infects, and to a re-emerging infection, meaning that the disease is increasing in frequency, either in its traditional geographic location or in a new area. Obvious examples of the former include swine flu and bird flu, as well as SARS coronavirus, all of which infected and spread among humans for the first time recently. A good example of a re-emerging infection is West Nile virus, which emerged on the eastern seaboard of the USA in 1999, having arrived from Israel, and then crossed the entire continent in just four years.
Newly discovered viruses which cause well-established diseases are also sometimes referred to as emerging infections. These include some tumour viruses. Novel viruses that emerge and spread successfully in a naïve host population produce an epidemic, defined as ‘an infection occurring at a higher than expected frequency’, and may progress to a pandemic if it is spreading on several continents at once. However, these definitions give no indication of the extent or duration of a disease outbreak. The differing patterns of emerging infectious disease outbreaks depend on a number of viral factors, including it blood and blood products (Hs incubation period and method of spread, and important host behavioural factors like living conditions, propensity to travel, and the success of any preventive measures. Both HIV and SARS emerged fairly recently, but the pattern of these outbreaks couldn’t have been more different. Whereas the SARS epidemic was short and sharp, all over in a few months, the HIV pandemic has lasted decades and is still ongoing.
SARS coronavirus first emerged in November 2002 in Foshan, Guangdong Province, China, where it caused an outbreak of atypical pneumonia. Initially, the virus spread locally, particularly among patients’ family members and hospital staff, but everything changed in February 2003 when a doctor who had treated SARS cases in Guangdong Province unwittingly carried the virus to Hong Kong. He stayed one night at the Metropole Hotel in Hong Kong before being admitted to hospital, where he died of SARS a few days later. In the hospital, the virus spread to staff, which sparked the Hong Kong epidemic. During his 24-hour stay in the hotel, the doctor transmitted the virus to at least 17 guests (apparently he sneezed in the lift), who then carried it to 5 more countries, thus spawning epidemics in Canada, Vietnam, and Singapore. This rapid dissemination of the virus threatened to cause a pandemic, but surprisingly by July 2003 it was over, the final toll being around 8,000 cases and 800 deaths involving 29 countries across 5 continents.
SARS coronavirus spreads through the air and causes disease in almost everyone it infects. After an incubation period of 2 to 14 days, victims develop fever, malaise, muscle aches, and a cough, sometimes progressing rapidly to viral pneumonia that requires intensive care, with mechanical ventilation in around 20% of cases. But with no known treatment or preventive vaccine, how was the epidemic conquered so effectively?
Left to its own devices, SARS coronavirus would undoubtedly have continued its trail of destruction but, fortunately, many of its characteristics played into the hands of those trying to stop it, and contributed to its speedy demise. Importantly, the virus mostly causes overt disease, with few unidentified silent infections. This meant that cases and their contacts could be recognized and isolated, and since victims are only infectious once the symptoms have developed, this prevented further spread. Also, as the disease is usually severe and debilitating, relatively few patients, excepting the doctor from Guangdong, travelled far while infectious. During SARS, the virus is produced in the lungs and spread by coughing. This generates relatively heavy mucus droplets that do not spread far through the air; hence close contacts like family members and hospital staff are mainly at risk, the latter constituting over 20% of cases worldwide. Once all these factors were appreciated, old-fashioned barrier nursing and isolation of patients and their contacts were enough to interrupt virus spread and prevent a pandemic.
Unlike SARS coronavirus, HIV has been spreading among humans since the early 1900s and despite drugs which control the infection, it is still on the increase in certain areas of the world. Currently, there are 33 million people living with. We now know that HIV, and it has caused over 25 million deaths since the first report of AIDS in 1981. It is interesting to examine the reasons for this lack of control, and to contrast these with the success of the SARS control programme.
Firstly, although SARS coronavirus had spread internationally by the time it was recognized by the World Health Organization (WHO), it had only infected humans for a few months. Compare this to the estimated 100 years during which HIV was silently creeping around sub-Saharan Africa, where poverty, wars, and poor health services conspired to facilitate its spread, and prevent the recognition of AIDS as a new disease.
Secondly, in contrast to SARS’ short incubation period and infectivity coinciding with overt disease, HIV has an average asymptomatic period of eight to ten years, and during this time the carrier may transmit the virus to any number of contacts.
Thirdly, the two viruses spread by completely different means. Whereas SARS coronavirus’s airborne flight can easily be intercepted, interruption of HIV’s transmission is more problematic. HIV spreads most commonly by sexual contact. Other routes of spread include mother to child during birth and breast feeding, in transplanted organs, transfused blood and blood products, and via contamination of surgical instruments as well as injecting drug users’ equipment. These non-sexual routes can in theory be interrupted, but they are almost insignificant in global terms compared to its spread via heterosexual contact. In exploiting the basic human urge to procreate, HIV targets the young and sexually active and is passed unwittingly from one apparently healthy host to another through sexual networks. Although its transmission can be halted by barrier devices, the vast amounts of money spent on the promotion of condom use for safer sex have not altered sexual practices sufficiently to halt the pandemic.
Untreated HIV infection leads to AIDS after a lengthy silent period, and this syndrome was first recognized in 1981 in San Francisco when several gay men died of unusual infections superimposed on severe HIV-induced immunosuppression. As the extent of the pandemic became apparent, three distinct risk groups emerged: people with multiple sexual partners, both heterosexual and homosexual; people with haemophilia or other disorders requiring regular infusions of blood or blood products; and injecting drug users. Utilizing the molecular clock technique to track back to the origin of HIV in humans, sub-Saharan Africa, particularly Kinshasa in the Democratic Republic of Congo (DRC), was pinpointed as the epicentre of the pandemic. Then using two early viruses isolated from people living in DRC, scientists have calculated that HIV has infected people in this region for around 100 years. They have identified a single virus strain that carried the infection from DRC to Haiti and another that transported the infection from Haiti to the USA. So by the time HIV was discovered in 1983, the pandemic was already growing exponentially and has proved very difficult to control.
A virus that jumps to a new host species for the first time has a series of hurdles to overcome before it can establish itself in the naïve population. Firstly, it must infect cells of the new host, and this involves finding a host cell receptor molecule to lock on to. Many would-be virus infections abort at this point, a fact that explains the species barrier of most viruses. Even if the new virus can unlock and enter host cells, it still may not be able to reproduce inside them, resulting in another abortive infection. For instance, HIV cannot infect mouse CD4 T cells because the molecular structure of the mouse CD4 molecule differs from the human equivalent in ways that make it unrecognizable to the virus. Even if mouse T cell socioeconomic groups in–0Ss are transplanted with the human HIV receptor molecules (CD4 and CCR5) in the laboratory, the infection is still abortive because mouse T cells lack the essential proteins that the virus requires for its replication.
However, on occasions viruses do enter and successfully replicate in cells of a new host species, but after a window of opportunity lasting about a week during which they can colonize the host and reproduce, their offspring must move on to another susceptible host before the developing host immunity wipes them out. SARS coronavirus and H5N1 (bird) flu have both managed to infect humans but differ in their success to date. Whereas SARS coronavirus can spread between humans, H5N1 flu, which first jumped from birds to humans in 1997, is unable to do so. This flu virus strain is still poorly adapted to its new (human) host, and we will be in danger of an H5N1 flu pandemic only once it evolves an efficient method of spreading between us.
Most apparently novel viruses that infect humans are not entirely new. They are either viruses that have mutated or recombined sufficiently to be unrecognizable by our immune system, or, more commonly, they have come from other animals, seizing the opportunity to hop from one animal species to another when the two come into contact. The latter are called zoonotic viruses, and the diseases they cause are zoonoses.
As we have seen, RNA viruses mutate much more frequently than DNA viruses, producing a variety of offspring, of which some can dodge host immunity more efficiently than their siblings and therefore flourish at their expense. Eventually, a virus emerges that is sufficiently different from its ancestors to be immunologically unrecognizable. Then everyone in the host population will be susceptible and it may cause an epidemic. Flu is a prime example of a virus that mutates frequently, a process called antigenic drift. The flu virus circulates constantly in the community, accumulating genetic changes and causing regular winter outbreaks and larger epidemics every eight to ten years. However, its story is actually much more complicated. There are three flu strains, A, B, and C, and flu A is a zoonotic virus. With the help of wild birds, this virus can also undergo recombination, or antigenic shift, producing an entirely new strain of flu in one go by exchanging fragments of its genome with other strains. This has the potential to cause a pandemic.
The natural hosts of flu A viruses are aquatic birds, particularly ducks, but the viruses also infect a variety of other animals including domestic poultry, pigs, horses, cats, and seals. Flu A replicates in birds’ guts and is excreted in their faeces, causing no symptoms but effectively spreading to other bird populations. Flu viruses have eight genes which are segmented, meaning that instead of its genome being a continuous strand of RNA, each gene forms a separate strand. The H (haemaglutinin) and N (neuraminidase) genes are the most important in stimulating protective host immunity. There are 16 different H and 9 different N genes, all of which can be found in all combinations in bird flu viruses.
Because these genes are separate RNA strands in the virus, on occasions they become mixed up, or recombined. So if two flu A viruses with different H and/or N genes infect a single cell, the offspring will carry varying combinations of genes from the two parent viruses. Most of these viruses will not be able to infect humans, but occasionally a new virus strain is produced that can jump directly to humans and cause a pandemic, as we have experienced recently with swine flu.
Over the last century, there have been five flu pandemics: in the H1N1 ‘Spanish’ flu of 1918, all eight genes came from birds; the H2N2 ‘Asian’ flu of 1957 acquired three new genes, including H and N from birds; and the H socioeconomic groups in–0S3N2 ‘Hong Kong’ flu of 1968 acquired two new genes from wild ducks. The ‘Russian’ flu of 1977, which probably escaped from a lab in Russia, was a 1950s version of H1N1; whereas the H1N1 ‘swine’ flu which appeared in Mexico in 2009 has six genes from North American and two genes from Eurasian pig flu viruses.
On average, flu A epidemics and pandemics kill around one in a thousand of those infected, with the very young, the very old, and those with chronic diseases being particularly at risk. Pandemics additionally often target young adults: in the 1977 Russian flu pandemic, the young were hardest hit because they had no previous immunity, whereas most older people were spared as they were already immune. Similarly, in the recent swine flu pandemic the disease was most severe in young adults and pregnant women. However, by far the most virulent flu virus on record is the 1918 pandemic strain which targeted young adults and killed 40–50 million people worldwide, around 2.5% of all those infected.
With the virulent H5N1 bird flu on the horizon, the late 1990s saw a flurry of activity aimed at finding out why the H1N1, 1918 flu was so deadly. Amazingly, researchers managed to reconstruct the virus using samples taken from a flu victim buried in the permafrost in Alaska, and from post-mortem lung samples from a US serviceman stored in a pathology laboratory for some 80 years. Compared to nonpandemic H1N1 virus, the 1918 strain has several mutations that enhance its infectivity and growth rate in human cells. In particular, a mutation in a gene called NS1 prevents virus-infected cells from producing interferon, the key cytokine for preventing virus spread and triggering the whole immune cascade. This allows the virus to get a head start, and in some cases the body responds with an uncontrolled outpouring of cytokines, called a cytokine storm. A massive and inappropriate inflammatory response ensues that may cause death from respiratory failure as the victim’s lungs fill with fluid. This mutation is already present in the H5N1 bird flu virus, accounting for the high mortality rate among those it infects. Fortunately, it has not learned to spread between humans so far.
The transfer of ‘new’ zoonotic viruses from their primary host to humans can be facilitated by certain behaviours or cultural practices, and we now know that a particular risk is our interaction with wild animals, many of which carry viruses with the potential to infect us. Both HIV and SARS coronavirus were introduced into the human population when their natural hosts were hunted and killed for consumption.
It is now clear that HIV-like viruses have jumped from primates to humans in central Africa on several occasions and that one of these viruses, HIV-1 type M, has succeeded in spreading globally.
The ancestor of this virus has been traced to a subspecies of chimpanzees (Pan troglodytes troglodytes), among whom it can cause an AIDS-like disease. Since these animals are hunted for bush meat, it is most likely that human infection occurred by blood contamination during the killing and butchering process. This transfer took place some 100 years ago, probably in southeast Cameroon where the chimpanzees carrying the virus most similar to HIV-1 type M live. Scientists postulate that the virus (inside humans) travelled from Cameroon along the Sangha River, a tributary of the Congo River, to reach Leopoldville (now called Kinshasa), then the capital of the former Belgian Congo, from where it spread globally.
SARS coronavirus also entered the human population from an animal food source, this time in the live animal markets of China. Here, there are a number of small mammals on offer and several, most noticeably the Himalayan palm civet cat, c socioeconomic groups in–0Sarry SARS-like viruses. As the natural reservoir of SARS coronavirus has now been identified as the fruit bat, it is presumed that the virus transferred to other animal species in markets where they are packed into overcrowded cages, and then jumped to the market traders.
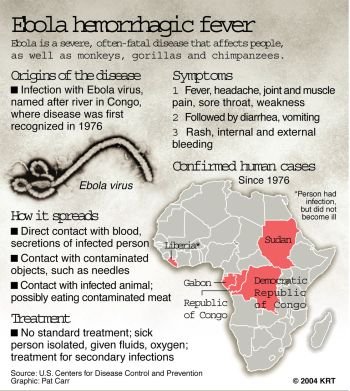
SARS is not the only potentially lethal virus carried by bats; several bat species are reservoirs for viruses that have recently jumped to humans. In fact, bats almost certainly transmit the much-feared and highly infectious Ebola and Ebola-like viruses.
Epidemics of Ebola viral haemorrhagic fever hit rural populations in central Africa from time to time, and these outbreaks have increased in frequency in DRC, Gabon, and Sudan since the mid-1990s. Ebola virus was discovered after an explosive outbreak in Yambuku, a remote village in northern Zaire (now DRC), in 1976, and was named after the local Ebola River. This epidemic began with a school teacher who developed a headache and fever after returning from a trip into the bush. He was treated for malaria at the local mission hospital, but his symptoms progressed to a full-blown viral haemorrhagic fever with soaring temperature, severe abdominal pain, diarrhoea, vomiting, muscle cramps, and generalized bleeding. He died within a few days. The virus, transmitted by direct contact with the patient and his body fluids, then spread to his family, other hospital patients, and staff, eventually infecting 318 people in the village and killing 280 of them.
Counter-intuitively, control of Ebola outbreaks is quite straightforward once the disease is recognized. Since the infection is so debilitating, few infected victims move far from the outbreak site, and once the person-to-person chain of infection is broken by strict barrier nursing and isolation of cases and contacts, it can be rapidly controlled. Unfortunately, the virus has recently jumped to large apes, particularly chimpanzees and lowland gorillas. This not only threatens the very existence of these endangered species, but also provides an additional transmission route to humans when they come into contact with these animals, perhaps accounting for the recent reported rise in outbreaks.
Another dangerous bat-transmitted virus emerged in 1997 when a group of Malaysian farmers reported a respiratory disease outbreak among their pigs, and later several pig farmers and abattoir workers came down with encephalitis. Fortunately, the disease did not spread directly from person to person, and was later controlled by slaughtering over a million pigs in 1999. Sadly, by this time, there had been 265 cases of encephalitis with 105 fatalities. A novel paramyxovirus was isolated from a victim’s brain and named Nipah virus after the village in which he lived. The virus was traced to fruit bats, and its trail to humans probably began when a colony of bats was left homeless by deforestation.
The bats relocated to trees near the pig farms and the virus spread to the pigs via bat droppings, and then from the pigs to the farmers and abattoir workers. Due to our invasion of their territories, bats and humans are coming into contact with increasing frequency. The Nipah virus turns out to be very similar to bat-borne Hendra virus, isolated in 1994 from the victims of an outbreak of severe respiratory disease on Hendra farm in Brisbane, Australia, where it killed 14 horses and one of their trainers. Similar outbreaks in West Bengal in 2001 and in Bangladesh in 2001 and 2004 are also attributed to bat viruses, indicating that these cute, furry animals are far from safe companions. Several insect species act as virus vectors, ferrying them from one host to another, so that any changes in vector population density directly affect transmission of these viruses. Ever since 2004, when the use of the insecticide DDT (dichloro-diphenyl- around 5,000 to 10,000 years agoes6Ptrichloroethane) was restricted by the Stockholm Convention on Persistent Organic Pollutants, mosquitoes in certain tropical and subtropical areas have undergone a population explosion. This has led to the reemergence of several mosquito-borne microbes, including dengue virus. Traditionally restricted to South-East Asia, dengue virus has been spreading to new geographical areas for the last 60 years, and is now a major problem in tropical Africa and South America.
Dengue virus often infects without causing symptoms, but it may cause classical dengue fever, characterized by a rising temperature; severe headache; muscle, bone, and joint pains; vomiting; and a skin rash. For obvious reasons, the disease is dubbed ‘break-bone fever’, but although unpleasant, full recovery is the rule. However, in 1–2% of cases this progresses to dengue haemorrhagic fever, with bleeding into the skin, gastrointestinal tract, and lungs leading to circulatory failure – called dengue shock syndrome. With no specific treatment, the syndrome has a high mortality.
Bluetongue virus is another insect-borne microbe that has socioeconomic consequences since it infects domestic animals, mainly sheep, and is spread between them by midges. Once infected, sheep develop fever followed by excessive salivation, frothing at the mouth, nasal discharge, and swelling of the face and tongue. The bluish tinge to the sheep’s tongue, caused by low blood oxygen levels, gives the disease its name. Lameness is another symptom, and pneumonia may develop which can prove fatal. More often, a slow recovery ensues, but impairment of wool growth is an important commercial consequence.
Bluetongue was first recorded in South Africa and has traditionally been restricted to tropical and subtropical areas where it also infects cattle and goats, although with milder symptoms than in sheep. Its geographical distribution reflects the fact that African midges cannot survive severe winters. However, thanks to global warming, the midge has recently extended its territory into southern Europe, where the virus has been picked up by hardier European midges. Each year, the insects undergo a population explosion in early summer, when transmission of bluetongue virus peaks. Bluetongue has been moving steadily northwards and was recorded in Germany, France, Holland, and Belgium in 2006 where it survived the winter, and reached the UK and Denmark in 2007, Sweden in 2008, and Norway in 2009. So will the midge’s unwelcome passenger virus survive these northern climes, become indigenous, and affect domestic animals? Only time will tell.
With these examples of emerging and re-emerging infections in mind, we can now address the question of why they are presently on the rise in both humans and domestic animals. Many modern-day lifestyle factors increase our risk of emerging infections, and most of these are linked to overpopulation. The world’s population approximately doubled every 500 years between the beginning of the Christian era and 1900, when it reached 1.6 billion. But in the 20th century, life expectancy rose steeply and the population quadrupled, hitting 6 billion by 2000. If this growth rate continues unabated, we are set to reach 9 to 10 billion by 2100.
A population of this size brings many problems, not least diminishing natural resources, increasing pollution, loss of biodiversity, and global warming. But as far as emerging virus infections are concerned, the most acute problem is literal around 5,000 to 10,000 years agoes6Ply lack of space. We have already seen how invading the territories of wild animals, be it to chop down the rain forest, hunt for food, or extend our cities, risks acquiring unknown, sometimes lethal, viruses. With over 50% of us now living in megacities, like Tokyo with over 35 million inhabitants, viruses, once acquired, find it very easy to spread between us. This is particularly so among poor city dwellers in resource-poor countries, with the inhabitants of shanty towns living in cramped, unhygienic shacks where the lack of fresh air and clean water, and absence of sewage disposal, provides easy access for microbes of all sorts. As illustrated by HIV, SARS, and swine flu, successful local spread soon leads to international dissemination. With over a billion people worldwide boarding international flights every year, novel viruses have an efficient mechanism for reaching the other side of the world within 24 hours.
Animal viruses also thrive on overpopulation. For them, intensively farmed animals equate to crowded cities and present the opportunity to spread easily among their hosts. A dramatic example is the foot and mouth disease virus outbreak in Britain in 2001 when pyres of slaughtered farm animals were seen all over the countryside. The virus, which is highly infectious among cattle, sheep, pigs, goats, and deer, is widespread in Asia, Continental Europe, Africa, and South America, but generally absent from Australasia, the USA, Canada, and the UK. It targets the skin around the mouth and hooves, leading to lameness, and although not usually fatal, the loss of condition it produces in infected animals is very economically damaging.
Animal viruses usually cross international boundaries unnoticed inside their hosts, and sometimes jump to humans on arrival at their new destination. As we have already seen, West Nile fever virus jumped from Israel to the US in 1999, although its mode of transport remains a mystery. The virus naturally infects birds and is spread among them by mosquitoes, which can then infect humans via a bite. The infection is usually asymptomatic but may cause a flu-like illness and, very occasionally, encephalitis. To date, the virus has not passed from person to person.
Epidemics and pandemics
Once an acute emerging virus such as a new strain of flu is successfully established in a population, it generally settles into a mode of cyclical epidemics during which many susceptible people are infected and become immune to further attack. When most are immune, the virus moves on, only returning when a new susceptible population has emerged, which generally consists of infants born since the last epidemic? Before vaccination programmes became widespread, young children suffered from a series of well-recognized infectious diseases called the ‘childhood infections’. These included measles, mumps, rubella, and chickenpox, all caused by viruses, of which only chickenpox remains widespread in the West today.
To find out when and how humans first experienced these acute childhood infections, we need to look back some 10,000 years to the farming revolution that began in the Fertile Crescent (the area between the Rivers Tigris and Euphrates, in modern-day Iraq and Iran) and spread rapidly to neighbouring lands. This dramatic alteration in lifestyle, which was later adopted independently in several other parts of the world, converted our ancestors from nomadic hunter-gatherers to farmers living in fixed communities. The consequences of this change with respect to the microbes that infected them were equally dramatic. It led to a period of ever-increasing epidemics of severe and often lethal infections caused by microbes, including those that we now recognize among the acute childhood illnesses.
This onslaught was directly related to the change in lifestyle. Temporary camps were replaced by tiny, cramped, permanent dwellings in crowded villages, allowing airborne microbes easy access to their hosts; while food and water, previously collected daily, were now stored in unhygienic conditions, enhancing faecal–oral transmission of gut-infecting microbes. The major factor in introducing new microbes to the early farmers was their close proximity to recently domesticated animals that now shared their dwellings, and which carried their own private microbial zoos.
The molecular clock technique shows that smallpox virus is most closely related to the pox viruses of camels and gerbils, and not to cowpox as was previously supposed. Scientists think that the rodent pox virus probably jumped to humans and camels in the early farming period, estimating that the event took place sometime between 5,000 and 10,000 years ago. In contrast, measles virus’s closest relative is Rinderpest virus, the cause of cattle plague, and scientists calculate that the two viruses diverged from a common ancestor around 2,000 years ago. So it seems that these and many other animal microbes infected humans when they first came into close contact during the early farming era. These were the emerging viruses of the period and, as is the way with most emerging infections, at first each epidemic began with transfer of the virus from animal to human host and ended when most susceptible people in the population were infected. Then, as trading links between villages, towns, and countries expanded, these ‘new’ viruses followed along, causing ever larger and more widespread epidemics.
Studies on measles virus outbreaks in island populations to induce immunity without severeindenthanging3eapublishof varying sizes, such as Iceland, Greenland, Fiji, and Hawaii, have been used to estimate the minimum population size required for the virus to circulate continuously in a community, as opposed to it being introduced from outside, at the beginning of each epidemic. The results show that a population of around 500,000 is sufficient, a figure that is probably similar for other airborne viruses. We know that the first towns of this size evolved around 5000 BC in the Fertile Crescent, and so from this time onwards, viruses like measles could break the link with their animal hosts to become entirely human pathogens.
Viruses spread between hosts in many different ways, but those that cause acute epidemics generally utilize fast and efficient methods, such as the airborne or faecal–oral routes. The former is the most efficient method of spread in industrialized nations where people tend to live in crowded towns and cities, whereas this is outstripped by the latter in non-industrialized countries, particularly where standards of hygiene are low.
Broadly speaking, virus infections are distinguished by the organs they affect, with airborne viruses mainly causing respiratory illnesses, like flu, the common cold, or pneumonia, and those transmitted by faecal-oral contamination causing intestinal upsets, with nausea, vomiting, and diarrhoea. There are literally thousands of viruses capable of causing human epidemics, but only a few cause distinctive childhood diseases like measles, mumps, chickenpox, and, until quite recently, smallpox.
Airborne viruses
Smallpox virus is in a class of its own as the world’s worst killer virus. We know that it first infected humans at least 5,000 years ago and killed around 300 million in the 20th century alone. The Antonine plague, which began in AD 166, is thought to represent the first ever smallpox pandemic. The plague hit the Roman Empire during the reign of Emperor Marcus Aurelius Antoninus, who ruled over an area encompassing most of modern-day Europe, the Middle East, and North Africa. It began in Seleucia, a city on the River Tigris, while Roman soldiers were suppressing an uprising, and as they returned victorious to Rome, they carried the virus with them, broadcasting it along the way. Over the next 20 years, smallpox raged like a plague throughout the Empire and beyond to India and China, and killed 5,000 a day in Rome at its height. The Romans believed that the plague was punishment meted out by the gods for the sacking of Seleucia, particularly for the opening of a sealed tomb in the temple of Apollo. Marcus Aurelius’s physician, Galen of Pergamum, described a ‘fever plague’ inducing severe thirst, vomiting, and diarrhoea, as well as a rash of fever blisters that were dry, black, and ulcerating – very suggestive of smallpox.
From this time on, smallpox produced ever-increasing epidemics as towns and cities grew and became more crowded. The virus killed up to 30% of those it infected, scarring and blinding many of the survivors. But after centuries of devastation, smallpox virus was finally eliminated from the wild in 1980.
Until the 1960s, almost every child suffered from the classic childhood virus infections measles, mumps, and rubella, but following the introduction of vaccination programmes these have become a rarity in the developed world. All three viruses access the body through the nose and mouth and colonize the local lymph glands. Then, after a two-week incubation period, during which the victim is blissfully unaware of the invader growing inside them, the viruses travel in the bloodstream to internal organs. This viraemia induces non-specific symptoms like fever, malaise, headache, and runny nose cross the placenta as each virus homes to its particular target organs and the characteristic signs of the illness appear: the tell-tale rashes of measles and rubella, and the painful, swollen parotid glands of mumps. These diseases may be mild in most cases, and recovery leads to lifelong immunity, but each is associated with severe complications that make their prevention worldwide an essential goal.
Of the three viruses, measles is the most infectious and produces the severest disease. It killed millions of children each year before vaccination was introduced in the mid-20th century. Even today, this virus kills over 300,000 children annually in countries with low vaccine coverage. Most deaths from measles result from pneumonia, caused either by the measles virus itself or by other microbes invading the damaged lungs. In developing countries, measles kills 1–5% of those it infects, but this may reach 30% in severely overcrowded living conditions such as refugee camps. The high mortality has long been assumed to be due to pre-existing malnutrition and other debilitating diseases such as malaria, but recent studies in Guinea-Bissau pinpoint another risk factor. They found that measles mortality was higher in rural areas where there are longer intervals between epidemics. This means that rural children experience measles at an older age than urban children. During a rural epidemic, more children per household are susceptible and are often infected sequentially, one from another, in a single epidemic. In this situation, mortality is higher in the second and third child to be infected than in the first (index) case. The reason is that measles virus is mainly spread by droplets generated by coughing, and it is most infectious over short distances in enclosed spaces. Thus, in this study, scientists argued that the index case most probably acquired the virus outside the home, where a low infecting viral dose is likely to result in a relatively mild illness. In contrast, the dose would be higher in the second family member infected from the first because of a cramped and crowded home. And if the more severe the infection, the more virus produced by sequential sufferers, then the dose received would escalate in the family chain along with the disease severity.
Because humans are the only host for measles virus, and the vaccine is safe and highly effective, measles eradication is feasible, and indeed has been achieved in the US, UK, and Australia over prolonged time periods. The Measles Initiative of 2001, set up with the eventual goal of worldwide measles elimination, had already reduced global measles deaths by 74% worldwide by 2005, mostly by increasing vaccine coverage in sub-Saharan Africa and the Eastern Mediterranean and Western Pacific regions. Now the immediate aim is to prevent 90% of measles deaths worldwide and to eradicate the virus by 2020.
Rubella is commonly called German measles because it was first described by a German doctor, Friedrich Hoffmann (1660–1742), in the 18th century, and it was distinguished from measles and scarlet fever by another German doctor, George de Maton, in the 19th century. The infection is generally mild, short-lived, and often passes unnoticed. It would be of little importance if that were the end of the story, but in the 1940s an Australian physician, Norman Gregg (1892–1966), noticed an association between rubella in pregnant mothers and congenital defects in their infants, commonly heart and eye abnormalities and hearing loss. Rubella virus in the mother’s blood crosses the placenta and grows in the baby, whose immune system is too immature to respond. This damages the baby’s developing organs, and the risk period coincides with organ formation between 10 and 16 weeks of pregnancy. Rubella vaccine is generally given along with measles and mumps vaccines in the MMR. Vaccine preparation, and has virtually eliminated congenital rubella in countries where vaccine coverage is high, but the condition remains a problem in developing countries. Mumps is also a relatively mild disease, particularly in childhood, when it may, like rubella, pass unnoticed. Vaccination is advised to prevent the severe complications of meningitis, encephalitis, and orchitis (inflammation of the testis). The latter develops in around 30é of males who catch mumps after puberty and is often bilateral, a condition that may lead to infertility.
Chickenpox is still rife in the UK, and is one of the commonest acute childhood infections worldwide. It rips through children’s nurseries and schools on a regular basis, infecting almost all susceptible children before moving on. However, an effective vaccine is available and is given to all children in the US, Canada, Australia, and some European countries, but is not used routinely in the UK. Although chickenpox behaves like a classic acute infectious disease analogous to measles, mumps, and rubella, the virus remains in the body for life after the initial infection and may later resurface to cause shingles.
Most people get two or three colds a year, suggesting that the immune system, which is so good at protecting us against a second attack of measles, mumps, or rubella, is defeated by the common cold virus. But this is not the case. In fact, there are so many viruses out there that cause the typical symptoms of blocked nose, headache, malaise, sore throat, sneezing, coughing, and sometimes fever, that even if we live for 100 years, we will not experience them all. The common cold virus, or rhinovirus, alone has over 100 different types, and there are many other viruses that infect the cells lining the nose and throat and cause similar symptoms, often with subtle variations. For example, unlike most respiratory viruses that spread best in the winter months, coxsackie viruses often cause summer colds, and echo- and adenoviruses may produce additional sore red eyes, a condition called conjunctivitis. All these viruses produce local symptoms after two or three days’ incubation period that last three to four days and require no treatment. However, infection often leads to loss of work or study time, and because the infections are so common, the global economic burden is enormous.
As any parent knows, young children are very prone to upper respiratory tract infections – the familiar ‘snotty-nosed kid’. They are susceptible to the large number of respiratory viruses circulating in the community at any one time, and although most infections are mild, any of these viruses can cause more severe disease, particularly in infants. An infection that spreads to the lower bronchial passages causing bronchiolitis, pneumonia, or croup can be alarming and may require hospital treatment.
Viruses such as parainfluenza and respiratory syncytial virus are particularly associated with these problems in infants, regularly causing epidemics and a peak in hospital admissions. Indeed, worldwide acute respiratory infections, mostly viral, cause an estimated four million deaths a year in children under. Anyone who confidently states that they have been off work for a few days with ‘the flu’ is likely to have suffered from one of the many cold-causing viruses, but a genuine attack of flu caused by influenza A or B is quite a different matter. Although producing similar respiratory symptoms, flu has more severe constitutional effects with additional aching muscles and fever, often lasting for seven days. Even after recovery, sufferers may feel lethargic and depressed for a while, further delaying their return to work. In temperate climates, flu A and B outbreaks occur most winters, with significant mortality, mainly from pneumonia, among the very young, very old, and those with other debilitating diseases. Furthermore, the economic burden through loss of work time and hospital admissions is great enough for governments to seek preventive and curative strategies.

{kind=link}