What is ANGIOPLASTY and STENTING?
Heart Disease Treatment With Angioplasty and Stents
What is thrombolytic therapy and when is it used?
Patient comment:
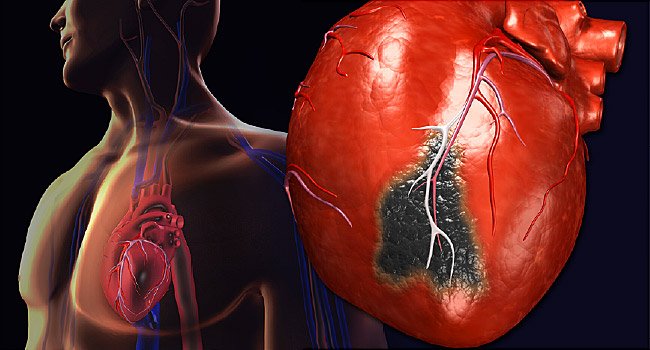
When you suffer from a heart attack, the most important medication is thrombolytic agent (a drug to dissolve blood clots blocking your heart arteries). This thrombolytic agent is most effective when given within 30 minutes to 3 hours after the onset of a heart attack. That’s why you should not delay seeking medical attention as soon as you feel like you are having a heart attack. If the agent is given more than 24 hours after the beginning of the symptoms, it does you almost no good at all.
Thrombolytic therapy is the intravenous administration of medications that dissolve blood clots blocking your coronary arteries. The thrombolytic agents are often called clot busters. The earlier you receive a thrombolytic agent after a heart attack, the greater your chance of survival. That’s because reducing the damage of your heart muscle leads to improved pumping action.
Thus, thrombolytic therapy is a mainstay in the early management of heart attack at the present time. For best therapeutic results, the thrombolytic agent must be administered within 30 minutes to 3 hours after the onset of symptoms. Giving the agent later than 3 hours reduces the beneficial effects of thrombolytic therapy. Delaying such treatment for 12 to 24 hours drastically reduces the therapy’s beneficial effects.
In addition, if the agent is administered after more than 24 hours from the onset of symptoms, thrombolytic therapy produces little or no beneficial effect.
At present, the most important and standard thrombolytic drug is tPA or alteplase (Activase) in the United States. The next most commonly used thrombolytic agents are retoplase (Retavase), urokinase (Abbokinase), and finally streptokinase (Kabikinase, Streptase). In addition, other thrombolytic agents may include lanoteplase, anistreplase, and tenectoplase (the newest drug).
A thrombolytic drug, most commonly alteplase, is given intravenously with an anticoagulant agent (e.g., heparin). Heparin and aspirin are unable to destroy existing blood clots, but they can prevent blood clots from reforming after they are broken up.
Certain limitations govern who the best candidates are for thrombolytic therapy. For example, you would have had to experience symptoms of acute heart attack within 3 hours after their onset (within 12 hours at most). Also, if you are an adult younger than 75 years and have an S-T segment elevation on an ECG, you are considered a good candidate. If as a heart attack victim you had a systolic BP of less than 180 mm Hg, any heart rate, and diabetes, you would qualify.
In some clinical circumstances, your doctor would avoid thrombolytic therapy or use it with great caution. If you were older than 75 years, you’d be at a higher risk, even if you were otherwise in good general health. Then, too, such therapy would not be used if your heart attack symptoms had continued for more than 12 hours. The same precaution would apply to you if you were pregnant. Your doctor might hesitate to use thrombolytic therapy, or use it cautiously, if your ECG demonstrated no S-T segment elevation, even if the diagnosis of a new heart attack were certain.
Others who would prompt caution are those with recent trauma (especially head injury) or surgery, heart attack victims recovered from prolonged CPR, and those with active peptic ulcers.
Thrombolytic therapy would not be used at all in treating those with recent major bleeding from any organ or for those whose ECG demonstrated a depressed S-T segment, such as seen in a non-Q wave heart attack. Doctors would avoid using such therapy also for treating people with a history of stroke, particularly cerebral hemorrhage, and those with uncontrolled and extremely elevated high BP.
As long as the above-mentioned conditions are not present, thrombolytic therapy should be considered as the first-line lifesaving measure for any heart attack victim, regardless of age or gender.
Terms:
Clot busters – another term for thrombolytic agents, medications that dissolve blood clots.
Cerebral hemorrhage – a form of stroke with hemorrhage (bleeding) in the brain.
The earlier you receive a thrombolytic agent after a heart attack, the greater is your chance of survival.
Does thrombolytic therapy produce complications?
Fortunately, complications and side effects from thrombolytic therapy are rare. Hemorrhagic stroke (cerebral hemorrhage) is the most serious complication of thrombolytic therapy, and it usually occurs during the first day after the administration of the agent. The chances of this occurring are reported to be 0.5 to 0.1%. In addition, internal bleeding may occur in other organs, such as the intestines, stomach, and urinary tracts. Other side effects may be allergic reactions to the agents, hypotension (low BP), and cholesterol embolization.
Streptokinase (one of the thrombolytic agents) given without heparin is reported to show the lowest risk of complication. However, its effectiveness in restoring blood flow is less than that of other thrombolytic agents. The mortality (death) rate from bleeding is reported to be 3 in every 1,000 patients treated with thrombolytic therapy, but its survival benefits, particularly in combination with aspirin, last for many years.
Other aspects of managing a heart attack include percutaneous transluminal coronary angioplasty (PTCA), coronary artery bypass graft (CABG), an artificial pacemaker, electric shock treatment, and cardiopulmonary resuscitation (CPR). Another new device called an atherectomy catheter can shave off and remove plaque from the inside of the diseased coronary artery. A new device called a laser-tipped catheter can vaporize the blockage of the diseased coronary artery with a tiny laser beam. This new device may be useful when the blocked or narrowed segment of the diseased coronary artery is long, and the ordinary PTCA is technically difficult to perform.
Term:
Cholesterol embolization – cholesterol clot formation in the bloodstream
What is coronary angioplasty, and who needs it?
Coronary angioplasty (an abbreviated term for percutaneous transluminal coronary angioplasty or PTCA) is one of two standard revascularization procedures to open up the narrowed (stenotic) or blocked coronary arteries. Emergency coronary angioplasty is the more commonly performed procedure for practically all heart attack patients. Coronary angioplasty is most successful when performed within 12 hours after the onset of symptoms, and the sooner the better. A cardiac surgical team must be available immediately in case the PTCA is unsuccessful and produces major complications.
After injecting a local anesthetic into the groin (less frequently in the arm), doctors place a narrow tube (catheter) containing a fiber optic camera and direct it to the narrowed or blocked coronary artery. Then they pass a tiny deflated balloon through the catheter to the narrowed or blocked coronary artery as they watch an x-ray image on a TV screen. They advance the guide catheter in the diseased coronary artery until it arrives at the blockage. At that point, they inject a small amount of contrast material through the catheter, watching the procedure on the screen, to determine the exact location of the blockage or narrowing of the coronary artery.
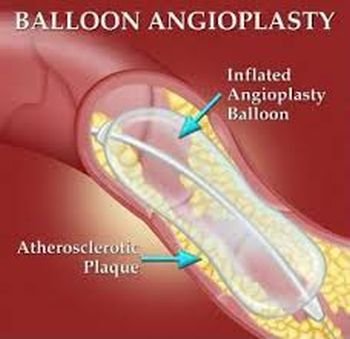
They then inflate the small balloon to squeeze the plaque against the walls of the coronary artery. That action flattens out the plaque and opens up the narrowed artery so that it will be able to restore blood circulation.
The doctors inflate the balloon for perhaps 30 to 120 seconds and then deflate it. Chest pain often occurs when the balloon is inflated because the blood flow is temporarily interrupted by the balloon in the segment of the heart muscle. Medical staff should be informed as soon as a brief chest pain occurs. They inflate and deflate the balloon several times thereafter.
Doctors sometimes use a relatively new device called a coronary stent, an expandable metal mesh tube. They commonly implant the stent during PTCA-about 80% of angioplasty procedures-at the site of the blockage to prevent restenosis of the coronary artery.
When the PTCA is considered to be successful, doctors remove the balloon catheter and perform a coronary angiogram (visualization of coronary arteries by movie camera) to assess the improved coronary blood circulation.
Then they remove the guide catheter. Most patients are able to go home by 1 to 2 days after the procedure.
Terms:
Transluminal coronary angioplasty (PTCA) – standard revascularization procedure to open up narrowed or blocked coronary arteries.
Coronary stent – expandable metal mesh tube used in PTCA to prevent restenosis of the coronary artery.
{kind=link}