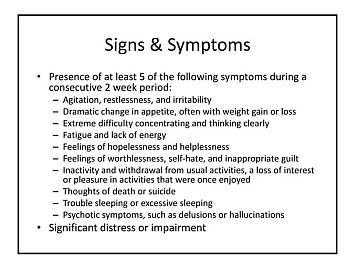
Teen Depression: Signs, Symptoms and Getting Help
Going into hospital
I have been referred to a hospital specialist. I am not keen to see them. Do I have to go?
No, but remember that NHS resources are scarce. Your doctor will not refer you to a specialist lightly. Do go to the appointment if this has been arranged. If you are not clear why your doctor wants to refer you, do ask.
If you are still unwilling to go to the appointment, please let the outpatient clinic staff knows early. They can then offer the appointment to someone else.
Admission
Admission is suggested in less than a quarter of those being seen by a specialist. This suggestion will not be made lightly and means that there are serious concerns. Admission is very likely to be advised if there is a risk of suicide, or if the depressive illness is causing someone to eat and drink inadequately. Admission may be advised to enable treatment to be established quickly.
If the depressive illness seems to be ‘resistant’ to treatment – perhaps two or three antidepressants have been tried with poorresults – a brief admission can enable an intensive review of treatment to take place. This review will include checking that no physical illness is present that may be contributing to the depression.
Sometimes admission is necessary in order to give a specialised treatment such as ECT (electroconvulsive therapy), which is necessary in a small minority of cases. Although ECT can safely be given to you as a day patient, there may be medical reasons, to do with the anaesthetic, for the doctors to suggest inpatient care. People who are older and frail, or have a medical illness like diabetes or heart disease, are more likely to be offered inpatient ECT than treatment as a day patient (see the ECT section later).
What happens when I am in hospital?
You will be thoroughly reviewed and details of your history – or details of the illness – will be taken. If you have been ill before, it will be important that the doctor knows what treatment you have had in the past – what has helped before is likely to help now.
Details of your family history of psychiatric disorder will be taken. The events leading up to the episode will be reviewed. Details of your medical history will be taken.
Physical examination
You will have a physical examination and this will include checking over your whole body, taking your blood pressure and pulse, listening to your heart and lungs, and examining your abdomen. It will also include examining your nervous system – looking in your eyes with an ophthalmoscope, checking your muscle power and tone, checking for sensation, and tapping your reflexes.
Only rarely is a serious physical illness found at this stage – something which has been silent, or missed before. These checks do need to be done.
Tests
Following this physical examination, or perhaps because of something that alerts the doctor in your history, other investigations are sometimes indicated. These may include an ECG (electrocardiograph), chest X-ray, or EEG (electroencephalograph).
If there have been marked problems with memory, this may be formally tested by a psychologist. Some routine blood tests will be taken – physical illness can show itself via mental illness or at least contribute to it.
The routine blood tests that are done are:
• Full blood count: to check for the presence of anaemia, or signs of infection;
• Urea and electrolytes: which give a good indication of kidney function;
• Thyroid function test: the thyroid gland either slowing down or speeding up may cause mood disorders;
• Calcium levels: high levels of calcium are a rare, but treatable cause of psychiatric illness;
• Liver function tests: if these results are abnormal it could indicate liver disease – which may cause depression or lethargy. Sometimes abnormal results will be the first pointer to the fact that there has been excessive alcohol use. It can be difficult and embarrassing to be open about the amount of alcohol used. Alcohol is a powerful depressor of mood – it can cause depression. Alcohol may have been taken in a vain attempt to try and feel more relaxed and brighter in mood;
• Occasionally, folic acid in red cells and vitamin B12: low levels of vitamin B12 as in pernicious anaemia, can cause depression and lethargy before other things start to go wrong. Sometimes levels of folic acid and vitamin B12 may be low because of excessive drinking of alcohol.
A sample of your urine will be taken. This will be tested to see if there is glucose, protein, or blood present. Each of these substances can indicate an underlying illness that couldcontribute to the depression (or, rarely, be causing it). Urine may also be screened for street drug use. The results are confidential – nobody will be contacting the police.
You will be weighed. A lot of depressed people lose weight because of loss of appetite. A rise in weight after admission is a sign of progress. Sometimes people overeat when depressed, and they may need help dealing with this. Weight on admission is a good baseline measure.
Treatment in hospital
When these basic investigations and tests have been done, a care plan is made. This is a treatment plan addressing your particular problems. A care plan involves an assessment by the doctor and the nursing staff. You will be allocated a ‘keyworker’ or professional on the ward, to set aside time to see you on a one-to-one basis. The keyworker is usually a nurse, but could sometimes be an occupational therapist, social worker, or psychologist.
A programme or timetable of daily activity will be put together. This may include group therapy, occupational therapy (treatment through activity) and physiotherapy. Physiotherapists are skilled in the teaching of relaxation techniques as well as having knowledge of a large range of therapeutic activity. You are also likely to have drug treatment that can be monitored closely on the ward.
Your care plan will discussed with you. It is a plan for your care so does ask questions. When you are well enough, day leave, then weekend leave, may be arranged to see how you cope outside the hospital. If all is well following a good leave, a target date to leave hospital is made. If it has been difficult to cope outside the hospital, it is a good opportunity to address those difficulties and try to ease them before trying leave again.
How can I keep in touch with my family whilst in hospital?
During your stay you will of course be able to see visitors. You may want to go off-site for a while with a visitor. Always ask staff first – they may otherwise waste valuable time looking for you. Staff may suggest you do not go out initially because it can be unsettling, or you may just have been started on medication, the effects of which are yet to be seen.
On returning to the ward after a trip out, staff might ask to search you or your bag or to breathalyse you. This is a common hospital practice and is done to try and ensure that you and your environment are as safe as possible. Alcohol and street drugs are strictly banned from hospitals. Objects that could cause harm are also as restricted as much as possible when somebody is very low in mood.
Tell your relatives your timetable so that they are not waiting about whilst you are having a treatment session. Relatives can phone the ward to ask how you are. No confidential information will be given out without your permission. You are, of course, entitled to refuse to see visitors. If you are visiting someone in the hospital and you are worried about anything that they tell you (perhaps for example about harming themselves), do tell a member of staff. Never assume everybody knows already. Two messages are definitely better than none.
Do I have to see medical students when I am in hospital?
No. You are entitled to refuse to see students. However, if you do agree, you are likely to be providing very valuable learning experiences for the student and you may well enjoy the contact. If you are an inpatient, a medical student may be allocated to you and become ‘your student’. They can provide another source of human contact and help while you are on a ward. It is an arrangement whereby both patients and students can benefit. A student talking to somebody who is depressed will learn far more about the illness and how it affects people than she or he will ever learn from reading a text book.

{kind=link}