DIABETES – A MAJOR RISK FACTOR FOR KIDNEY DISEASE
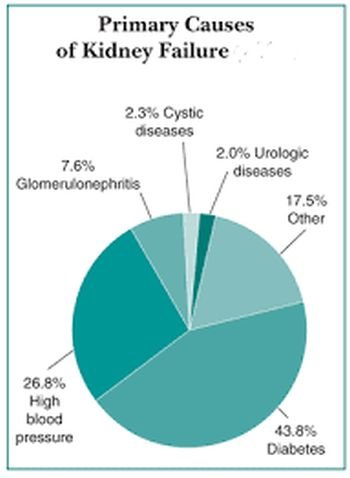
Kidney damage
It’s bad enough having diabetes. If I’m at risk also of kidney damage, what should I look for?
There are several ways in which diabetes may affect the kidneys, and they will show up in the routine urine and blood tests that you have at your diabetes clinic. A lot of glucose in the urine puts you at risk of infection that can spread from the bladder up to the kidneys (‘cystitis’ and ‘pyelo-nephritis’). Occasionally long-standing kidney infections may cause very few symptoms and are only revealed by routine tests. People with long-standing and poorly controlled diabetes are at risk of damage to the small blood vessels supplying the kidney just as the retina of the eye may be affected. This does not produce any symptoms but will be picked up on a routine urine test carried out at the diabetes clinic. Most clinics now use a special test for detecting ‘microalbuminuria’, which as the name implies is a microscopic amount of albumin (protein) in the urine. This is a useful test as it can pick up the earliest signs of kidney damage.
With more severe kidney disease, large amounts of albumin may be lost in the urine. This may make the urine froth and lead to a build-up of fluid in the body, which in turn leads to swelling around the ankles (oedema). Kidney failure may eventually develop in people who have had long-standing kidney problems.
This is usually picked up by blood tests and urine tests years before the symptoms develop.
I have developed kidney failure. Will be possible to have dialysis or even a transplant although I have diabetes?
Yes. The majority of people who are unfortunate enough to end up with kidney failure are suitable for both forms of treatment.
Dialysis (or chronic renal replacement therapy) is of two major types. The older type is haemodialysis where the blood is washed in a special machine twice a week; the more recent is a type of dialysis known as CAPD (chronic ambulatory peritoneal dialysis) where the fluid is washed in and out of the abdomen on a daily basis. People with diabetes seem to be very good at learning this method, which in some ways is simpler and cheaper than haemodialysis.
Transplantation is the aim of most dialysis programmes, but the supply of suitable kidneys is a limiting factor. The source of kidneys is from either people dying accidentally or live related donors who have agreed to give one of their two normal kidneys to a relative with kidney failure. A normal person can manage perfectly well with one kidney without any shortening of life provided that the kidney does not get damaged. The donor will, of course, have to have an operation and will be slightly more vulnerable as a result because they will have only one kidney to rely on instead of two.
I was found to have protein (albumin) in my urine when I last attended the diabetes clinic – what does this mean?
If it was only a trace of protein, it may mean nothing, but you should get your urine checked again to make sure it remains clear. If it is a consistent finding, it suggests either that you could have an infection in the bladder or kidney (cystitis or pyelonephritis) or that you have developed a degree of diabetic kidney damage (nephropathy). There are many other causes of protein (albumin) in the urine and it may not be related to your diabetes. If the protein in your urine is a consistent finding, it will need to be investigated, and you should ask to be kept informed of the results of the tests.
At my last clinic visit, I was told that I had microalbuminuria. What is this?
The very earliest stage of diabetic kidney disease leads to a leak of very small amounts of protein (albumin) into the urine. If it is a consistent finding, it suggests that your kidneys have been damaged by diabetes. If this is the case, then attention to control of your blood glucose and treatment of any tendency towards raised blood pressure is of great importance, as this can stabilise or even reverse the condition.
Nerve damage
There are various conditions that can affect the nervous system of someone with diabetes: diabetic neuritis, diabetic neuropathy, autoimmune neuropathy and diabetic amyotrophy.
I have been on insulin for 3 years. Eighteen months ago I started to get pains in both legs and could barely walk. Despite treatment, I am still suffering. Can you tell me what can be done to ease this pain?
There are many causes of leg pains, and only one is due specifically to diabetes. This is a particularly vicious form of neuritis – in other words, a form of nerve damage, which causes singularly unpleasant pain, chiefly in the feet or thighs, or sometimes both. The pain sensation is either one of pins and needles, or of constant burning, and is often worse at night causing lack of sleep. Contact from clothes or bedclothes is often acutely uncomfortable.
Fortunately, this form of neuritis is rather uncommon and always disappears, although it may take many months before doing so. Very good control of your diabetes is important as it will help to alleviate the symptoms and speed their recovery.
Relief is otherwise obtained by good painkillers, as recommended by your doctor, and sometimes assisted by sleeping tablets. Always remember that eventually recovery occurs, as otherwise, you will find that it is easy to get despondent. Also remember that the diagnosis must be made by a doctor who will consider all the various causes of leg pains before coming to a diagnosis of diabetic neuritis.
I have had diabetes for many years but my general health is good and I am very stable. During the last year, however, I have developed an extreme soreness on the soles of my feet whenever pressure has been applied, e.g. when digging with a spade, standing on ladders, walking on hard ground or stones, even when applying the accelerator in the car.
If I thump an object with the palm of my hand, I suffer the same soreness. The pain is extreme and sometimes lasts for a day or so. Could you tell me if you have heard of this condition in other people and what is the reason for it?
These symptoms may be due to diabetic neuropathy, a condition of damage to the nerves, which occasionally occurs in long-standing diabetes. It affects the feet more often than other parts of the body and often produces painful tingling or burning sensations in the feet, although numbness is perhaps more common. Strict control of your diabetes is important for the prevention and treatment of this complication – it can be made worse by moderate or high alcohol consumption.
I have diabetes controlled on diet alone. I suffer from neuritis in my face. My GP says there is no apparent reason for this but I wondered if it had anything to do with my diabetes.
Not necessarily, as there are a number of types of neuritis that can affect the face, which have absolutely nothing to do with diabetes? Examples include both shingles (herpes zoster) and Bell’s palsy, although, of course, both these conditions can affect people with diabetes.
There are forms of diabetic neuritis that do affect the face: one from occasionally affects the muscles of the eye leading to double vision, while another form can cause numbness and tingling. There is also a very rare complication known as ‘gustatory sweating’ where sweating breaks out across the head and scalp at the start of a meal.
I have recently been told that the tingling sensation in my fingers is due to carpal tunnel syndrome and not neuropathy as was first thought. Can you please explain the difference?
In carpal tunnel syndrome (which commonly occurs in people who do not have diabetes), the nerves supplying the skin over the fingers, the palm of the hand and some of the muscles in the hand get compressed at the wrist. Occasionally injections of hydrocortisone or related steroids into the wrist will relieve it, or it may require a small operation at the wrist to relieve the tension on the nerve. This usually brings about a dramatic relief of any pain associated with it and a recovery of sensation and muscle strength with time.
Diabetic neuropathy more commonly affects the feet than the hands and is usually a painless loss of sensation starting with the tips of the toes or fingers and moving up the legs or arms. It is only occasionally painful and may be difficult to treat. It is due to some form of generalised damage to the nerves, not to compression of any one nerve.
I have had diabetes for 27 years and have developed a complaint called bowel neuropathy. Please, can you explain what this is and what the treatment is?
Bowel neuropathy is one of the features of ‘autonomic neuropathy’, which may occur in some people with long-standing diabetes where there is a loss of function of the nerves supplying various organs in the body. In your case, the nerves that regulate the activity of your bowels have been affected. The symptoms include indigestion, occasionally vomiting, and episodes of alternating constipation and diarrhoea. Occasionally the episodes of diarrhoea are preceded by rumblings and gurglings in the stomach and sometimes this responds to a short course of antibiotics.
Otherwise eating a high-fibre diet is encouraged to prevent constipation. Irritable bowel syndrome can cause symptoms, not unlike this – it has nothing to do with diabetes, although it may occur in people with diabetes. If there is ever passage of blood or mucus within your stools, you should seek medical advice without delay.
The calf muscle in one leg seems to be shrinking. There is no ache and no pain. Is this anything to do with diabetes?
I have been taking insulin for 30 years. You do not mention whether you have noticed any weakness in this leg. Occasionally diabetic neuropathy can affect the nerves, which supply the muscles, in such a way that the muscle becomes weak and shrink in size without any accompanying pain or discomfort. It sounds as if this may be your problem. I have had diabetes for many years and have developed pain in my legs. My thighs, in particular, are very weak and wasted. I have been told that I have ‘diabetic amyotrophy’ Will it get better?
Diabetic amyotrophy is a rare condition causing pain and weakness in the legs and is due to damage to certain nerves. It usually occurs when diabetes control is very poor, but occasionally affects people with an only slight elevation of the blood glucose. Strict control of diabetes leads to its improvement but it may take up to 2 years or so for it to settle. The nerves affected are those usually supplying the thigh muscles as in your case, which becomes wasted and get weaker.


{kind=link}