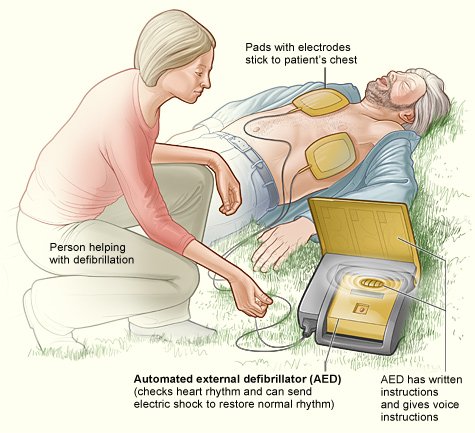
How to use an AED, Automatic External Defibrillator
Automated external defibrillators: Do you need an AED?
What Is an Automated External Defibrillator?
What is an automatic external defibrillator, and who needs it?
Patient comment:
If you are considered to be a high-risk patient after recovering from a heart attack, it is an excellent idea to keep an automatic external defibrillator (AED) in your home, especially when you had suffered from several episodes of cardiac arrest in the past. The AED is relatively easy to learn how to operate for anybody, and the device is not too expensive.
An automatic external defibrillator (AED) is a portable defibrillator that can deliver an electrical shock to halt ventricular fibrillation (very rapid, chaotic, and ineffective heart rhythm arising from the lower heart chambers). The AED is a small portable defibrillator that any lay person can easily operate. It’s used before you reach the hospital emergency room (ER). Because ventricular fibrillation must be stopped within a few minutes, an AED can prevent sudden death if used immediately.
Most ambulance teams carry an AED, as do many police and fire rescue units. In addition, AEDs are available in reputable commercial airplanes and various public places, such as sports arenas, large music halls, large international airports, and convention auditoriums. In addition, keeping an AED is highly recommended in private homes for high-risk patients recovering from recent heart attacks. High risks would be seen in those who have had multiple heart attacks, blockage of many coronary arteries, cardiac arrest (ventricular fibrillation), or massive heart muscle damage.
Such risks also would include the likelihood of future heart attack, cardiac arrest, or a history of serious complications.
What is an implantable cardioverter-defibrillator, and who needs it?
Recently, the use of implantable cardioverter-defibrillators (ICDs) has been increasingly popular among high-risk heart attack victims. Such a device can prevent sudden death from ventricular fibrillation.
The ICD is a small electronic device that can deliver an electrical shock automatically when you develop ventricular fibrillation or ventricular tachycardia (rapid and regular rhythm arising from the ventricles). New ICDs provide overdrive pacing to convert sustained ventricular tachycardia and backup pacing for very slow heart rhythm (bradyarrhythmia). The ICDs also provide various other sophisticated functions: noninvasive electrophysiologic (EP) testing and storage of detected arrhythmias.
An ICD consists of two main parts: a pulse generator and leads. The pulse generator is a small lightweight metal case (about the size of a pager or a small match box) containing a small computer and a battery. A surgeon implants the pulse generator under the skin near your left collarbone, usually under general anesthesia. (Some medical centers use local anesthesia and use general anesthesia for shock testing.) The leads are insulated, flexible wires placed in your heart, and they carry electrical energy from the pulse generator to your heart. The surgeon threads most leads from the ICD through one of your veins to the inside of your heart.
The surgery to implant the ICD takes about 2 to 3 hours. Most patients stay in the hospital for 1 to 2 days after the surgery. The cardiologist carries out an electrophysiologic study (EPS) before discharging you to check the device and to evaluate how your ICD is functioning. The cardiologist usually performs a post surgery EPS and subsequent studies noninvasively through the device via radio waves.
The cardiac team programs and designs each ICD specifically for individual need by performing an EPS before, during, and after the ICD surgery. In that way, your device can retain specific and individualized instructions about your needs. Programming of an ICD uses radio waves, and adjustment of the device can be made externally. An ICD monitors the electrical activity of your heart continuously on a beat-to beat basis, and it can effectively terminate ventricular fibrillation or tachycardia within seconds.
About 400,000 deaths occur each year in America from sudden cardiac arrest caused by ventricular fibrillation. Most patients who experience this are high-risk heart attack victims. High risk in heart attack victims has been identified previously (see the discussion of automatic external defibrillators). In particular, heart attack victims who survived cardiac arrest belong in the high-risk category. As has been stated, all patients with multiple heart attacks, blockage of multiple arteries, massive heart muscle damage, and major complications are at high risk.
What will I feel after an ICD implantation, and what should I do if I receive an electrical shock?
After your ICD implantation, like most patients you will experience some pain and stiffness around the incision area; it may remain swollen and tender for a few weeks. Your surgeon will prescribe some pain medications, but you should avoid any pain medication containing aspirin. If you respond like most patients, you will be discharged from the hospital 1 to 2 days after the surgery. Then you should receive full instructions regarding the functions of your ICD, care of the incision area, physical activity, medications, and various precautions and follow-up visits. Before you are discharged, you will be given an ICD identification card. It contains all necessary information about your ICD: Instructions in case of an emergency, your doctor’s name and phone number, and so forth. You should carry this card at all times.
A range of feeling is possible when your ICD is working for rapid heart rhythms. If you developed a rapid heart rhythm, the leads immediately would transmit signals to your ICD to initiate the electrical shock treatment. If the rapid heart rhythm were mild and short in duration, short and rapid electrical pulses would be delivered in a predetermined (programmed) pattern to restore your normal heart rhythm. Such electrical pulses are mild and, like most patients, you wouldn’t feel them.
If a very fast abnormal heart rhythm continued, however, your ICD would deliver a much larger electrical shock to terminate the rapid rhythm. Large electrical shocks will be painful, but the discomfort lasts only a fraction of a second. The discomfort is often described as a “kick in the chest.”
If you receive an electrical shock, you should sit down or lie down in whatever position you feel more comfortable. A family member or a friend should stay with you throughout the incident. If you were found unconscious, a family member or a friend should call an ambulance and your physician. If the electrical shock seems to be ineffective and the rapid heart rhythm continues, someone should inform your doctor immediately. Dialing Ambulance urgency might be necessary if you needed any urgent treatment. If your ICD seems to be working properly in response to a rapid heart rhythm, calling your physician immediately isn’t necessary. Your ICD will record and save all necessary information regarding the electrical shock therapy events. The information retrieved from the ICD is very important in evaluating your clinical conditions, the nature of your abnormal heart rhythms, and the effectiveness of your ICD. Thus, medical staff can adjust or reprogram your ICD if necessary to improve its effectiveness.
Term:
Automatic external defibrillator (AED) – portable defibrillator that can deliver an electrical shock to stop ventricular fibrillation.
A large shock is often described as a “kick in the chest.”
Keeping an AED is highly recommended in private homes for high-risk patients recovering from recent heart attacks.
{kind=link}