The following initial measures apply to all stroke patients. They are necessary to stabilize and assess the patient, and prepare for definitive therapy. All current and, probably, future stroke therapies for both ischemic and hemorrhagic stroke are best implemented as fast as possible, so these things need to be done quickly. This is the general order to do things, but in reality, in order to speed the process, these measures are usually dealt with simultaneously. They are best addressed in the ED, where urgent care pathways for stroke should be established and part of the routine.
6.1 Airway – breathing – circulation (ABCs)
. O2 via nasal cannula (routine oxygen delivery in ischemia might improve outcome).*
. Intubation may be necessary if the patient shows arterial oxygen desaturation or cannot ‘‘protect’’ their airway from aspirating secretions. However, intubation means that the ability to monitor the neurological exam is lost. The best approach in such patients is to prepare to intubate immediately, but before doing so, take a moment to be sure the patient does not spontaneously improve or stabilize with good nursing care (suctioning, head position, etc.). Also, if needed, use sedating or paralyzing drugs with a short halflife,
to allow for serial neurological exams.
. Consider putting the head of the bed flat. This can significantly help cerebral perfusion. The head of the bed may need to be elevated if airway protection and continued nausea and vomiting are concerns for those with obtundation, nausea, severe dysphagia, or aspiration risk.
. Consider normal saline bolus 250–500 cc if blood pressure is low.
. If the blood pressure is high, antihypertensive treatment is treated later.
6.2 What was the time of onset?
Determining the exact time of onset is critical for establishing eligibility for acute therapies, especially TPA. It is very important to be a detective. You will usually be told a time by the paramedics or ED triage nurse, but be sure to recheck the information you receive from them. If possible, try to speak personally with first-hand witnesses, nursing home staff, etc. Often paramedic information is based on an inexact estimate given to the paramedic when they arrive on scene, and then gets handed down as fact. You can often help establish the time of onset by finding out the time that the emergency call arrived at the dispatch center, and work backwards with the person who called. Other useful questions are to remind bystanders of their daily routine, TV shows, etc. that might help them accurately establish the time they found the patient or called the emergency services.
. In most cases, the onset is not observed – the patient is found with the deficit. In that case, or in patients who awakenwith symptoms, the onset time is the time the patient was last seen normal. However, if the patient awoke with symptoms, be sure to ask if the patient was up in the middle of the night for any reason (often to go to the bathroom) – as sometimes this puts the patient in the time window for treatment.
6.3 How bad are the symptoms now?
Examine the patient and do the NIH strokes scale (NIHSS).
The initial stroke severity is the most important predictor of outcome.
6.4 Do a non-contrast head CT
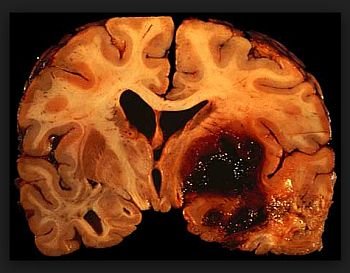
This will immediately rule out hemorrhage as blood is bright on a CT.
The initial head CT should not show obvious acute ischemic changes in patients with ischemic infarcts who are eligible for acute interventions, as acute ischemic changes become increasingly apparent between 3 and 24 hours.
The result will determine the first major branching point in therapeutic decision-making, to be covered later.
Obtaining the CT is often the major impediment in preparing for thrombolytic therapy, so efforts should be made to shorten ‘‘door to CT’’ time, which should be below 30 minutes.
For instance, we allow the triage nurse to order the CT scan if a stroke is suspected, and stroke patients will get preference over any other patient for CT access. Another problem is prompt reading of CT scans, especially in small hospitals in rural communities. Make sure to notify the reading radiologist that this patient is a possible TPA candidate.
. In some select centers, emergent MRI can be done very quickly and substitute for CT, but this is the exception. In general, MRI is deferred until after the first decision is made whether to treat with TPA. If the CT shows no blood, try to get the artery open.
6.5 If the CT shows no blood, try to get the artery open
TPA is the only FDA-approved treatment for ischemic stroke, and you should immediately begin to determine if the patient is eligible for this therapy, and prepare for its administration. The TPA protocol is detailed later.
6.6 Recommended diagnostic evaluation
The American Stroke Association guidelines list the following diagnostic studies for immediate use in a patient with suspected acute ischemic stroke.
These should be ordered in the ED, but you should not delay TPA treatment waiting for results once the patient meets established criteria.
6.6.1 All patients
Brain CT (brain MRI could be considered at qualified centers)
- Electrocardiograma
- Blood glucose
- Serum electrolytes
- Renal function tests
- Complete blood count, including platelet count
- Prothrombin time/international normalized ratio
- Activated partial thromboplastin time
6.6.2 Selected patients
- Hepatic function tests
- Toxicology screen
- Blood alcohol determination
- Pregnancy test
- Oxygen saturation or arterial blood gas tests (if hypoxia is suspected)
- Chest radiography (if lung disease or aortic dissection is suspected)
- Lumbar puncture (if subarachnoid hemorrhage is suspected and CT is negative for blood) electroencephalogram (if seizures are suspected)