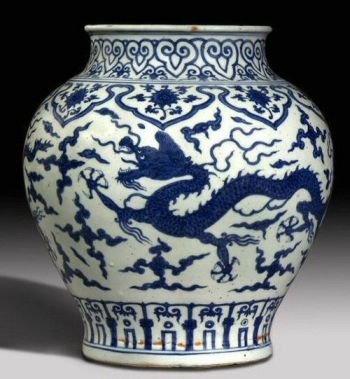
A certain amount of Porcelain was produced in the Yuan dynasty (1280-1368) decorated in underglaze blue. It was sometime, however, before the highly fashionable Celadon wares were overtaken by the these crisply decorated porcelains, which were initially seen as rather vulgar.
In 1368 the Mongol Yuan dynasty was overcome and the Ming dynasty was established. This lasted until 1644. During the early years of the first Ming Emperors reign, porcelain in underglaze blue or red was developed further. By the end of the 14th Century porcelain had reached fashionable status.
It would wrong to say that all porcelain from the Ming dynasty is worth huge amounts of money.
The output was enormous, many pieces were for export to the West and the survival rate has been high. Many of the wares that we have today were from the provinces rather than from the Imperial kilns and some were rather crudely potted and decorated. These pieces especially if damaged can be purchased for relatively modest amounts.
In the reign of Xuande (1426-35) superior wares were made in blue and white using a blackish blue glaze, also red was used. These superb wares were later copied in the 18th century; rather convincingly it has to be said. Later Ming period includes the coloured enamels of the Chenghua reign (1465-87). Blue and white was revived in the reign of Jiajing (1522-66), when overglaze red was added to the colours.
80% of reign marks on Chinese porcelain are retrospective, Intended as a tribute to Imperial ancestors. Square seal marks sometimes replace the more usual character marks. Reading from the top down, a six-character mark includes: character for “great”, dynasty, emperors first name, emperors second name, two characters meaning “in the reign of”. Pieces that bear the correct period mark ( catalogued “mark and period”) are obviously more valuable than those with retrospective marks.
***
When should I strongly consider the use of medications in my treatment?
The use of medication is always an option for someone symptomatic enough to seek mental health treatment. Several factors guide this decision, the first being the patient’s willingness to consider its use. Some patients will simply be too reluctant to consider medication for fear of side effects or fear of the loss of control that they perceive will occur from taking a pill that works on their mind. While these fears may make emotional sense to the anxious mind, and while an excess of any medication that works on the brain could create varying degrees of mental status changes, the primary goal of any carefully tailored medication regime is to gain more control over symptoms and unwelcome thinking patterns-or to have all of the desired effects without any of the side effects. Most patients, if uncomfortable enough with their symptoms and, in time, trusting enough of their doctor, will consider the use of a medication if they believe it might help lessen their distress. If you still are too scared to take a medication, do notpanic; you are a perfect candidate for psychotherapy with a doctor who specializes in the talking cure. Most patients have an internal threshold they live with. Something in their lives has tripped a circuit, putting them above that threshold and prompting them to go to a therapist for consultation. If you feel so overwhelmed that waiting to speak with someone feels like agony, you should probably be on medication. If your panic attacks are occurring regularly, if you cannot fly or leave your home, if your ability to work or take care of your family has become impaired, if your ability to read or concentrate has diminished, or if the feeling is one that your internal home has caught fire, then you should probably be on medication. Many pharmacologic strategies are shorter term, so trying a medicine does not have to mean months and months depending on a pill. It does mean making a commitment to feeling better and taking the leap of faith that your doctor will help you find a medicine that works for you. You and your doctor should be able to speak frankly about the risks and benefits of both taking medicine and not taking medicine, so as to help you make more of a free and informed decision.
What are the most common types of medications used to treat anxiety disorders, and what would the best kind be for me?
The main idea is to use a medicine tailored to your condition. If you have an accompanying depressive or manic-depressive picture, your doctor would address those conditions as well and strategize with you to use as few medications as possible. If cost becomes a real issue, you might want to consider medications available generically, such as the tricyclic antidepressants, which usually cause greater discomfort with their side effects. If you have particular issues with public performance, you might consider a beta blocker. Often two medications will be used together, such as a benzodiazepine and a Serotonin reuptake inhibitor (SRI). I think of the benzodiazepines as garden hoses that can be used to immediately water a garden while I think of the SRIs as longer-term sprinkler systems, with the anxiety disorder being like a drought. You may need to begin the watering immediately while also thinking ahead in terms of drought protection.
What do I need to know about the SRI medications?
The SRI medications serve as mainstays in the pharmacologic treatment of anxiety. They work well, safely, and broadly, and they usually address many underlying or accompanying symptoms of depression that may have stemmed from the anxiety. Most patients are able to experience symptomatic relief with a minimum of side effects, at least initially. The most immediate side effects-like headache, stomach upset, or sedation-are usually transient and manageable with ibuprofen or bismuth subsalicylate. Over the long run, side effects such as weight gain and/or sexual dysfunction may or may not become issues. Many patients do not gain weight for the first six months, if they gain it at all. At that time, the anxiety may be much better managed and responsive to psychotherapeutic intervention. Similarly, many patients will report some kind of sexual dysfunction, but many will not. Patients tell me the most about decreased libido, increased time to achieve orgasm, or inability to achieve orgasm. Depression also causes decreased libido, so many patients simply want to feel better and see if their sexual desire improves as a function of the depression’s lifting and wait to assess the potential side effects at that time. Some men already suffer from premature ejaculation, which makes the delayed time to orgasm a welcome side effect. Inability to orgasm as a function of the medication breaks the deal for most patients. Thankfully, there are alternatives that cause less sexual dysfunction but still treat depression.
A unique side effect that can go missed while taking an SRI is the induction of mania or hypomania. Characteristically, patients who have this side effect have a history of major depression and/or manic or hypomanic behavior from prior periods in their lives. The SRI simply elicits the elevated aspect of mood. However, there are patients who start to experience hypomanic signs just from the SRI, often at low doses and within the first week or two. Hypomanic behaviors include not needing to sleep as much, increasing euphoria and/or irritability, and feeling like one’s mind is moving more quickly than at baseline (mania is a more severe, longer lasting form of hypomania). A hypomanic person might also feel increasingly creative, sensual, sexual, or bubbly. Most patients with hypomania love it and wonder what the problem would ever be, but those people either do not know or have denied the danger of becoming frankly manic. Mania can endanger one’s entire career, marriage, and life via the grandiosity, recklessness, and lack of judgment with which it so often presents. Statistically, most patients receive an SRI from a well-intentioned but busy primary care doctor who prescribes it but cannot see the patient again for several weeks. In that time, the induction of hypomanic behavior can take place and can easily be missed by someone not trained to detect the subtleties of these early shifts.
Term:
SRI Serotonin reuptake inhibitor – A type of medication that is used to treat depression and anxiety by decreasing the rate at which serotonin is metabolized in the nervous system
{kind=link}