British Heart Foundation – Watch Your Own Heart Attack TV advert
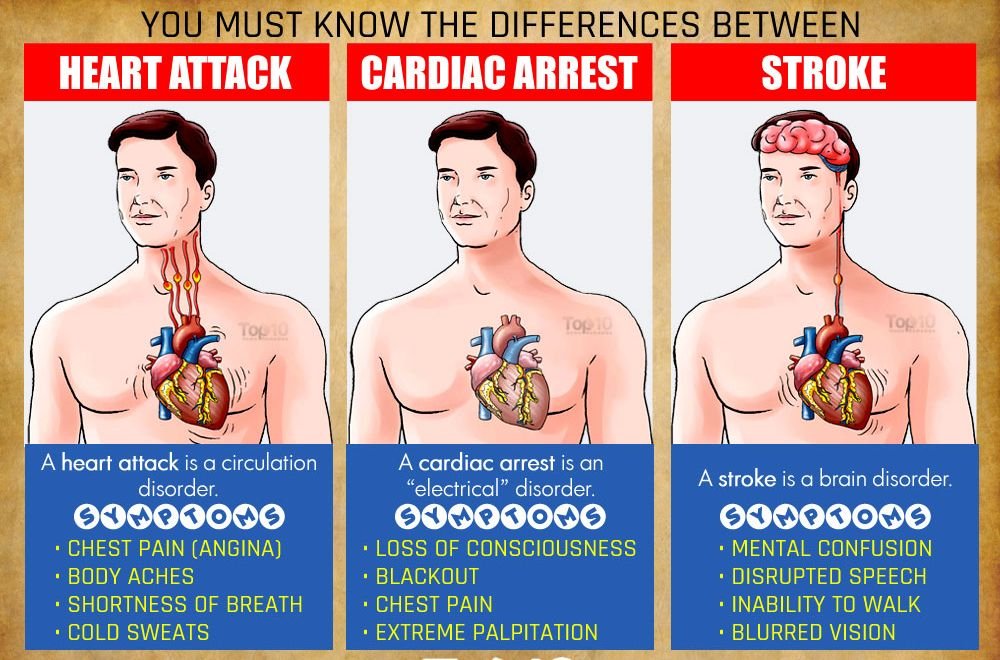
Warning Signs of a Heart Attack
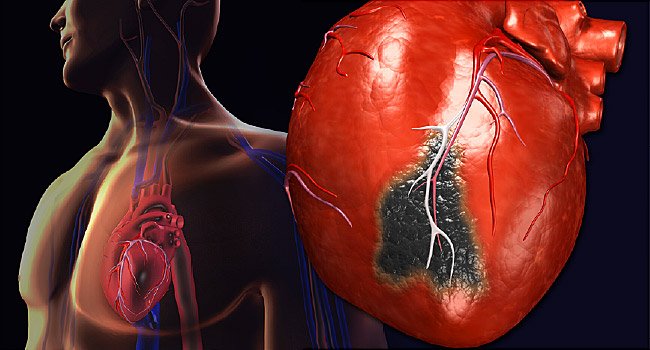
Heart Attacks and Heart Disease
What follow-up care and precautions should I take after I have an ICD implantation?
You should have close communication with your private physician after your ICD is implanted. Before being discharged from the hospital with your ICD, you will receive specific instructions on when to call your physician (or specially trained cardiac nurse).
Such instructions would specify calling within 24 hours of receiving an electrical shock; after two or more electrical shocks are received back to back; or if you felt any serious symptoms (e.g., dizziness, near syncope) from rapid heart rhythm lasting longer than 2 to 3 minutes.
Additionally, your instructions would tell you to call before scheduling any surgical or dental procedures and before scheduling any travel or moving to another location.
Naturally, you would call if you had any questions regarding your ICD, medications, or physical activities. Additional precautions to follow during the first few weeks after your ICD implantation are to avoid lifting anything heavier than 5 to 10 pounds, vigorous exercise or contact sports, and pushing, pulling, or twisting motions and to limit arm movements that may affect the electrical lead (wire) system. Also, you should keep cellular phones at least 6 inches away from your ICD and stay away from magnetic fields, such as high-voltage or strong electrical currents. You should avoid wearing any tight clothing that may irritate the skin over your pulse generator.
You should inform your physician of any signs of infection at the incision site or fever above 100°F. Finally, if any medical or dental care is needed, you should inform all medical and dental staff involved regarding your ICD. Implantation of your ICD requires periodic medical checkups to make certain that the ICD has been effective in halting all rapid heart rhythms. You should schedule follow-up visits several times a year at your doctor’s office or at a specially designed clinic dealing with ICDs. During such follow-up visits, medical personnel would use a programmer to guarantee that your ICD detects and treats rapid heart rhythms properly.
The programmer also can retrieve various medical information stored in the memory of your ICD. The medical information includes the events of any rapid heart rhythms to compare with your symptoms and your ICD’s effectiveness in handling such events.
Your ICD might need reprogramming according to changes in your medical condition and the effectiveness of the device for any rapid heart rhythms, particularly for life-threatening arrhythmias.
You need to replace your ICD’s battery every 5 to 8 years as well as the entire generator because its battery is sealed inside. Its battery life depends on the number of electrical shocks and the electrical energy used for stopping rapid heart rhythms. You should have the medical staff test the electrical leads and replace them as needed.
Resuming your daily activities should be gradual, according to your medical condition and your physician’s specific instructions. You should avoid driving a car for at least 6 months after being discharged from the hospital. The reason for this is the risk of ventricular arrhythmias (rapid heart rhythms from the lower chambers and not the risk of a problem in the ICD itself. Many patients who experience ventricular arrhythmias may need to avoid driving even after 6 months. Remember that you may develop dizziness, near-syncope, or syncope when ventricular arrhythmias occur. When you experience serious symptoms, you should have your physician evaluate you immediately, and your ICD may need reprogramming.
The natural increase in heart rate during sexual activity should not cause the ICD to deliver an electrical shock. If the ICD delivers an electrical shock during sexual activity, however, you should inform your physician immediately, because your ICD may need reprogramming.
If you schedule any travel, you should consult your physicians beforehand for proper instructions. You should request the name of a cardiologist and hospital in the area (other states or countries) to which you plan to travel. You are highly urged to carry a copy of medical records whenever you schedule an extended trip (longer than 1 month).
You should resume daily activities gradually. They may include walking, swimming, bicycling, bowling, gardening, cooking, golf, tennis, and returning to your previous job (desk job). You should refrain from such sports for the first 4 weeks, however, and any physical activity or emotional stress that may cause a very rapid heart rhythm. Needless to say, you should avoid vigorous or competitive sports and contact sports.
Lots of domestic appliances and devices create no interference with your ICD:
• Televisions, remote controls, tape recorders, radios, garage openers
• Kitchen appliances (toasters, blenders, electric can openers, microwave ovens, electric stoves, refrigerators)
• Washing appliances (electric washers and dryers) • Sleeping appliances (electric blankets, heating pads)
• Cosmetic appliances (hair dryers, electric shavers)
• Gardening appliances (lawn mowers, leaf blowers)
• Personal computers, printers, fax machines, electric typewriters, copying machines
• Machine shop tools (electric drills, table saws).
Certain other environments, activities, and equipment and devices can cause problems for your ICD:
• MRI (magnetic resonance imaging), radiotherapy, lithotripsy, electro surgery
• Magnetic fields (high voltage, strong electrical currents, large mechanical or industrial equipment)
• Strong magnets
• Large stereo speakers
• Battery-powered cordless power tools (screwdrivers and drills)
• Leaning over an uncovered running automobile engine
• Malfunctioning electrical or gas-powered appliances
• Being too close (closer than 6 inches) to a cellular phone. (Holding the phone to the ear opposite your implanted side is advisable.)
Your ICD identification card should be shown to airport security personnel because your ICD may set off airport security alarms. Most handheld metal detectors contain a magnet that may interfere with your ICD’s functions. Therefore, you should ask security personnel to limit scanning with such devices to less than 30 seconds over the site of the ICD or ask them to search you by hand if possible. At department store and library entrances, you may walk through most theft detection systems without harm.
What is catheter ablation, and who needs it?
Catheter ablation (or radio frequency ablation) is a nonsurgical treatment for many kinds of cardiac arrhythmias (abnormal heart rhythms) that are difficult to manage with various medications and other methods. When catheter ablation successfully corrects certain arrhythmias, the procedure is a permanent cure of a given arrhythmia.
The catheter ablation procedure will destroy parts of the abnormal electrical pathway (activity) causing a specific arrhythmia permanently. Thus, catheter ablation in many cases is effective for treating various types of rapid heart rhythms. During catheter ablation, doctors insert under mild local anesthesia a specially designed electrode catheter (a long, thin, flexible tube) into your heart via a vein in your groin or arm. Then they position the catheter in the area of the heart that’s causing a specific arrhythmia seen on an x-ray image. At the spot they determine is responsible for the arrhythmia, the electrodes at the tip of the catheter emit radiofrequency energy to destroy the small area of the heart tissue causing the arrhythmia. Catheter ablation is usually performed in conjunction with an electrophysiologic study (EPS, discussed in Question 60), and the procedure is extremely effective for certain arrhythmias when performed by well trained cardiac medical teams at well-equipped hospitals.
The procedure causes little or no discomfort and has a low risk of complications. However, since catheter ablation is an invasive procedure that requires the insertion of catheters into the heart, it does carry some small risks with some complications. You may develop bleeding at the insertion site, which could cause local swelling or bruising in the groin or arm. Some rare (but more serious) complications may include damage to your heart tissues and blood vessels, blood clot formation, and infection. If the procedure damages a normal electrical conduction system, you might need an artificial pacemaker.
For a few weeks after catheter ablation, you may experience occasional “skipped” heartbeats and palpitations. Although these symptoms are common, they are benign and self-limited events that will gradually disappear by themselves. However, you should inform your physician immediately if the rapid heart rhythm recurs or if some cardiac symptoms (chest pain, dizziness, shortness of breath, syncope or near-syncope) occur.
Like most patients, you would stay in the hospital overnight after the procedure and be able to resume your usual activities a few days after your discharge from the hospital. When catheter ablation is successful, the procedure will provide a permanent cure for many types of arrhythmias. Thus, the procedure can entirely eliminate a lifetime of many anti-arrhythmic agents (medications to treat various abnormal heart rhythms), leading to a healthy normal life.
What is cardiopulmonary resuscitation, and when is it used?
Patient comment:
Everyone should learn how to perform cardiopulmonary resuscitation (CPR), but it’s particularly important for family members who live with a heart attack victim. CPR is relatively easy to learn how to perform, and the CPR course is given by many local medical associations and hospitals.
Cardiopulmonary resuscitation (CPR) is urgently necessary when your cardiopulmonary system suddenly and unexpectedly fails to provide adequate and effective function. The purpose of CPR is to restore normal functions of the heart and lungs so that the delivery of adequate oxygen to vital organs—including the heart itself and the brain-is reestablished and maintained. Cardiac arrest most commonly occurs during the first few hours of a heart attack. Remember that permanent brain damage is a common end result when CPR is not applied within 4 minutes, even if cardiac function is restored later. In most cases, cardiac arrest and pulmonary arrest occur together, leading to cardiopulmonary arrest.
Those finding a presumed heart attack victim unconscious as a result of cardiac arrest should immediately seek emergency medical help and should apply CPR as soon as possible. A rescuer should not begin CPR until he or she has made sure that the victim is a) not breathing and b) has no heartbeat.
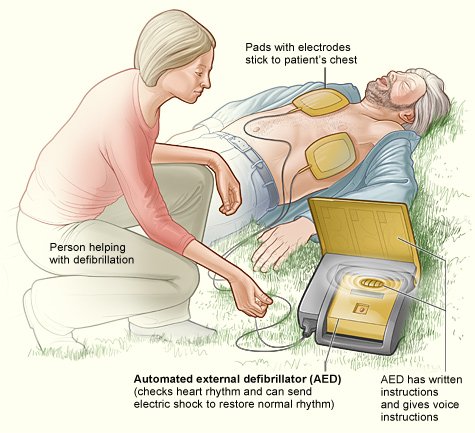
CPR performed on a person whose heart is beating can be harmful. The emergency line operator can give simple instructions over the phone on how to perform CPR, if no one seems to know the technique, until an ambulance arrives. As described earlier, the most common cause of cardiac arrest is ventricular fibrillation; hence, the use of an automatic external defibrillator (AED), if available, is a life-saving measure if used with performing CPR.
All medical and paramedical personnel must be fully capable of performing CPR. It is highly advisable for the general public to learn the proper technique for CPR because cardiovascular collapse is usually unpredictable. Family members of heart attack victims more urgently need a full understanding of CPR because cardiac patients have a much greater chance of developing cardiac arrest than do healthy people. The technique for CPR is relatively easy to learn, and the local Heart Association and many other medical organizations frequently give CPR courses.
Most hospitals in America commonly use the term code blue to designate cardiopulmonary arrest. A CPR team (consisting of specially trained physicians, nurses, and paramedical personnel) is on duty for immediate response to the code blue alert.
Cardiopulmonary arrest causes the loss of certain otherwise observable functions: consciousness (comatose state); pulse (no heartbeat); respiration (no breathing); heart tones (no heart sounds); and blood pressure (BP).
How CPR Is Performed
This rough guide to performing CPR should in no way take the place of CPR instruction. If you wish to be able to perform CPR, you should take a class from a certified instructor. However, the description below should provide you with a good idea of what is done in CPR and why it is done. Before you do anything else to help an apparent heart attack victim, call for help!
Your efforts may be in vain if you do not get the victim to a hospital quickly. CPR is a stop-gap measure only and is no replacement for prompt medical care. Your phone call to emergency is more likely to save the victim than any other action you take.
As stated, the purpose of the initial measure in CPR is to start and maintain the passage of air to the lungs so that adequate amounts of oxygenated blood can be delivered to all organs. Thus, the initial measure should follow the ABC guide: clearing the Airway (the route by which air travels to the lungs), starting and maintaining Breathing, and restoring blood Circulation.
As noted above, it is important to begin by making sure that the victim is incapable of breathing on his or her own, and to check for a heartbeat. In some cases, the victim may not be breathing, but still have heart activity-often ventricular fibrillation (VF), which is commonly associated with heart attacks. If VF is evident, those administering CPR should deliver a forceful blow to the sternum (around the breastbone) with the heel of the hand; they may repeat the blow once or twice more if that produces no response. A direct blow to the sternum can terminate VF and may restore normal heart rhythm. If this maneuver is not successful, however, help should immediately proceed to the next step.
Airway
The first maneuver in CPR should be to place the patient in a supine (lying down, face-up) position. The person performing CPR should place one hand behind the patient’s neck and the other hand on the forehead. When the head is tilted back, this maneuver lifts the tongue from the back of the throat so that the patient’s airway will be fully open. During this maneuver, the rescuer should remove any obvious foreign body in the mouth and airway. For many patients, this maneuver alone may be enough to restore breathing and to start recovery from cardiovascular arrest. The person providing CPR should put his or her ear over the mouth to listen for breath sounds. If the victim is breathing, no further direct action is required unless the breathing stops, but the victim should be continually monitored and transported to a hospital in an ambulance as soon as possible.
Breathing
If the victim is not breathing, CPR providers should maintain the backward tilt of the patient’s head with one hand and pinch the nostrils closed with the other hand. The rescuer should place his or her mouth over the patient’s mouth, completely sealing it to avoid any leak of air (Figure 12). At the end of inspiration (breathing in), one should exhale (blow out) a longer than – usual breath into the patient’s mouth. Artificial (mouth-to-mouth) respiration should be performed at a rate of 12 breaths per minute. If the technique is correct, a rise should be noted in the patient’s chest. If the chest does not rise, the rescuer should check again for blockages in the airway, make sure the nose is pinched, and readjust the mouth position to prevent leakage. There should be no loss of air through the nose or mouth as the lungs inflates. After inflation of the lungs, one should remove the mouth from the patient’s mouth, allowing the patient’s lungs to deflate. Air should be heard escaping from the lungs during that period. A pause of about five seconds should be enough to allow the lungs to deflate before the next breath.
The principle of mouth-to-nose resuscitation is essentially the same as that of mouth-to-mouth resuscitation. In this technique, while maintaining the backward tilt with one hand, the CPR provider should close the patient’s jaw and seal the patient’s mouth with the other hand. Then, one would place the mouth over the patient’s nose and, after inhaling deeply, would exhale into the patient’s nose. Artificial respiration should be performed at a rate of 12 breaths per minute.
Circulation
If the patient is not breathing and has no heartbeat (determined by feeling for a pulse in the neck or groin for about 5 seconds), the next step in the initial resuscitation measures is the application of cardiac massage. Closed-chest cardiac massage is recommended in practically all clinical circumstances except when the patient is already in the operating room or when chest wounds don’t allow closed-chest massage. To perform cardiac massage, the patient’s back must be placed on a firm surface. When the patient is on a soft surface (e.g., a bed), a hard board should be placed under the back. The reason for this is that you cannot compress the heart to pump blood adequately if the surface is soft under the victim. While standing alongside the patient, the rescuer places the heel of one hand over the lower third of the patient’s sternum; a common rule of thumb is to find the tip of the breastbone where the ribs meet and place your hand three fingers’ width up from that point. Only the heel of the hand should be in touch with the patient’s chest. The other hand may rest on the first hand.
The rescuer then compresses the patient’s chest 1.5 to 2 inches; the pressure should be smooth and uninterrupted. After that compression, the rescuer must release the sternum and ready the hand for the next compression. The duration of the chest compression should be similar to that of relaxation; that is, the amount of time spent doing the compression equals the time spent between compressions. The chest should be compressed about 60 times per minute and coordinated with artificial respiration. If only one person is present, 15 chest compressions are recommended, followed by two quick artificial respirations.
When two or more persons are available for CPR, every fifth chest compression should be followed by one lung ventilation (artificial respiration). To check the success of closed-chest cardiac massage, peripheral pulses (e.g., pulses on the neck or groin area) should be felt periodically-every minute or so-because, as stated above, if the rescuer is successful in restoring a heartbeat, the compressions should be halted. During the initial measures of CPR, one must check for several signs that indicate the success or failure of the resuscitative efforts. Important signs include pulse in the arm, groin, or neck arteries; heart tones (sounds); spontaneous breathing; and palpable or recordable BP. Of course, one should also be alert to any change in the patient’s neurologic status and in the status of consciousness.
When there is any evidence that resuscitative efforts have been successful, the rescuer may stop and observe the patient for several seconds. If the cardiovascular collapse has stopped, one should continue to observe the patient very closely. When resuscitative efforts have been successful outside a hospital setting, ambulance personnel should transport the patient promptly to a nearby ER. Needless to say, paramedic personnel of the ambulance will take over the CPR efforts as soon as they arrive at the scene. If, however, there is no change in the patient’s status, those in attendance must continue artificial respiration and cardiac massage until an ambulance arrives. They should not stop CPR for longer than 5 seconds.
After CPR
Various complications of closed-chest cardiac massage may occur, although the procedure is relatively safe in most instances. When treating children and elderly people, one must not be overly vigorous in chest compression to avoid any unnecessary damage to the ribs, sternum, and various organs. Complications of cardiac massage may include fracture of the ribs and sternum; hemothorax (bleeding in the chest cavity); hemopericarium (bleeding in the sac surrounding the heart); pneumothorax (collapse of the lungs); rupture of the stomach or the aorta (the largest arterial trunk); laceration of the liver and spleen; and bone marrow embolism (blood clots in the bone marrow).
After successful CPR, assessment of the underlying cause of the cardiopulmonary arrest is essential. Thus, the cardiac care unit (CCU) staff should closely observe and treat any patient who has recovered from cardiopulmonary arrest. First, they must manage the underlying heart disease (e.g., heart attack) together with the major complications (e.g., life-threatening arrhythmias, CHF, and the like). Some patients may require an implantable cardioverter-defibrillator (ICD), an artificial pacemaker, or various medications, depending upon the clinical circumstance.
Of course, the treatment of the underlying heart disease-heart attack-is essential. Thus, some patients may need coronary angioplasty or coronary artery bypass graft. It should be noted that after a massive heart attack, some patients may develop cardiopulmonary arrest again after recovery from their first arrest. Therefore, medical staff must monitor even more closely any heart attack victim with extensive heart muscle damage or multiple artery blockages.
Feature
Conversation with a Patient Recovered from a Heart Attack Mr. Benjamin Han is a 67-year-old retired banker (vice-president of one of the major banks) who had suffered from a heart attack 13 to 14 years ago and recovered from a heart attack without any complication. Coronary angioplasty was performed with a stent. His coronary risk factors included diabetes mellitus, abnormal blood cholesterol levels, occasional smoking, type-A personality, and some stress (job-related). His wife is a retired dentist. The following questions and answers are a candid conversation with the patient.
Q. What was the first symptom you experienced upon the onset of your heart attack?
A. On day 1, I experienced a short but severe pain in my left chest, and the pain was sharp enough to stop my routine daily walk outside of my office. I did not take it seriously at that time, but, in retrospect, it must have been a warning sign of the oncoming heart attack the next day.
Q. Did you feel any type of chest discomfort, significant shortness of breath, tingling sensation or numbness in the arms or shoulders?
A. Soon after lunch on day 2 on the way back to my office, I felt my breathing was short, uneven, and uncomfortable. My face was pale enough for co-workers to notice. My feeling then was that I must be having a not-so-unusual indigestion problem.
Q. Did you experience marked weakness, dizziness, or feeling of a fainting spell?
A. My pale face coincided with a sense of dizziness. I do not remember actual syncope, but I remember that I was not in a talking mood, as I felt weak and uncomfortable.
Q. What were you doing when you experienced any of the above-mentioned symptoms?
A. I was waiting in front of an elevator after walking back from my lunch. My walk was not at a routine pace, however.
Q. What action did you first take when you considered that you might be having a possible heart attack?
A. As I was returning to my office, my secretary first noticed my pale face and she commented on it. As she realized my weakness and my reluctance to converse with her, her friend who happened to be visiting her remarked that I must be having a heart attack. Her friend, I found out later, was a former nurse. Her suggestion was to go to the hospital. I hesitated initially, disbelieving what I heard. However, my secretary insisted on calling my personal friend, the cardiologist Dr. Edward Chung at Thomas Jefferson University Hospital, and I finally called Dr. Chung reluctantly.
Q. How soon did you go to a nearby hospital emergency room (ER)?
A. Upon hearing my medical history over the phone,
Dr. Chung considered strongly that I was having a heart attack, and he ordered me to call an ambulance and come to his hospital ER right away.
Q. What mediations were given to you in the ER and what diagnostic tests were performed?
A. I believe that I was given a thrombolytic agent (later found out that it was tPA-tissue plasminogen activator), and a series of blood tests with an ECG was performed.
Q. What additional diagnostic tests and treatment were performed when you were transferred to the CCU?
A. Cardiac catheterization with coronary angiogram (arteriogram) before performing coronary angioplasty.
Q. Was coronary angioplasty performed? How many blood vessels (arteries) were dilated?
A. My team of doctors performed coronary angioplasty on my left anterior descending artery. I had a second angioplasty on the same coronary artery with a stent implantation 6 months later because of restenosis. At that time, the use of a stent was somewhat experimental and not yet widely used.
Q. Was coronary artery bypass graft performed? How many blood vessels were treated?
A. No bypass surgery was performed.
Q. Did you suffer from any significant complications such as congestive heart failure and abnormal heart rhythms?
A. Fortunately, I did not have any complications.
Q. Did you experience angina (chest discomfort) or any other cardiac symptoms prior to this heart attack?
A. I might have experienced a sense of sluggishness and weak muscle strength. The briefcase I carried in the morning felt burdensome. But I did not know all these feelings were related to the heart attack. I do not recall any chest discomfort (angina) in the past.
Q. How long did you stay in the hospital?
A. It must have been for about 10 days. Hospital stay at the time was not restrictive.
Q. How many medications are you taking after your discharge from the hospital?
A. Initially, I was taking aspirin and atenol everyday. Later, I added a series of vitamins C, E, and folic acid. Now, I take two baby aspirins a day, folic acid, and Zocor (cholesterol-lowering drug).
Q. Are there significant changes in your lifestyle, diet, physical exercises, and coronary risk factors?
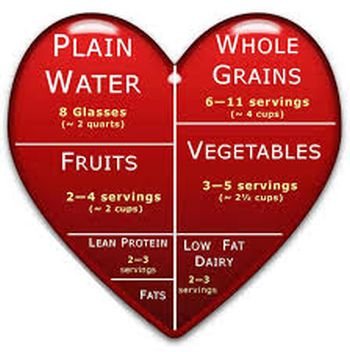
A. My wife has been very conscientious about my diet (e.g., lean meat, balanced healthy foods) Although I preferred high cholesterol foods, I have been listening to my wife’s advice 95% of the time. I have switched my regular exercise from tennis to golf, following my doctor’s recommendation. I have an exercise routine of walking three times a week and golfing three to four times a week. I have been very deliberate in all my efforts in minimizing stress-trying not be emotionally charged, and avoiding any cause of anxiety, if at all possible.
Q. Do you have any contributing risk factors (coronary risk factors) such as smoking, family history, high blood pressure, diabetes mellitus, high cholesterol, obesity, etc.?
A. Most of my siblings seem to have a history of high cholesterol, but none seem to show high blood pressure. I am the only one in my immediate family who has diabetes, which came to me in my early 50s. I must have had a stressful career and environment. I smoked irregularly and moderately before the heart attack. Since then, I quit smoking completely.
Terms:
Peripheral pulse – pulse in the arms or legs.
Hemothorax – accumulation or blood in the chest cavity.
Hemopericardium – accumulation of blood in pericardial sac.
Before you do anything else to help an apparent heart attack victim, call for help!
{kind=link}