IVMS-Adrenergic Physiology and Pharmacology for Medical Students
Adrenergic Receptors
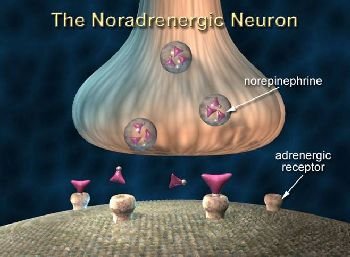
ALSO referred to as adrenoceptors, are a class of G-protein coupled receptors that are targeted by catecholamines. These receptors, found in peripheral tissue, initiate a “fight-or-flight” sympathetic nervous response when bound to their endogenous ligands.
Speciically, adrenergic receptors are targeted by the catecholamines epinephrine and norepinephrine (also known as adrenaline and noradrenaline, respectively). When the adrenal medulla releases these catecholamines in response to stress, the agonist-adrenergic receptor complex initiates responses including pupil dilation, energy mobilization, and blood diversion toward skeletal muscle, sweating, increased blood pressure, and increased heart rate.
There are several subtypes of adrenergic receptors. The two major classes include the alpha-adrenergic (α) and beta-adrenergic (β) receptors. α-adrenergic receptors bind norepinephrine and epinephrine. Β-adrenergic receptors link to G-proteins and initiate cAMP second messenger cascades when activated by catecholamine binding. Mediated by adenyl cyclase, β-receptor complexes work to increase the intracellular concentration of cAMP secondary messengers.
Adrenergic drugs stimulate the sympathetic nervous system directly by binding to an adrenergic receptor, or indirectly by stimulating norepinephrine release.
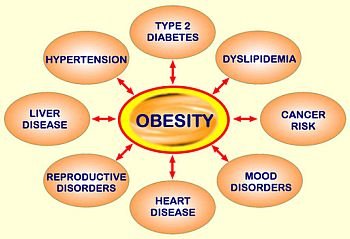
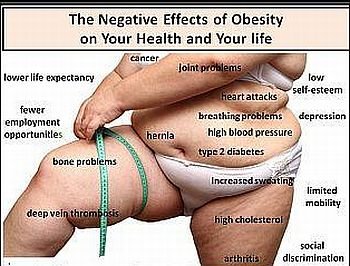
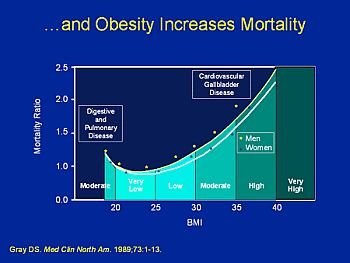
These drugs are commonly used as therapy against bronchial asthma, cardiac arrest, and allergic reactions, but also hold great pharmacologic potential as appetite suppressants and obesity drugs. If one considers that weight control is the delicate balance between central and peripheral factors, it is easy to see why adrenergic receptors are a current, exciting pharmacologic target for obesity. While satiety and appetite are regulated by the central nervous system, energy mobilization is a function of the peripheral nervous system.
The relatively new discovery of adrenergic receptors that control food cravings and energy expenditure suggests that obesity can be targeted both centrally and peripherally by the mediation of these receptors.
The most commonly investigated adrenergic receptors for obesity include the beta-3-adrenergic receptor and the 5-HT2C receptors. The β-3-adrenergic receptor, located in adipose tissue, regulates lipolysis and thermogenesis. It is now thought that this receptor plays a crucial role in weight control in humans, and a genetic mutation in the receptor has been identified to cause morbid obesity and type 2 diabetes.
This genetic receptor mutation is associated with the hereditary obesity seen in the Pima Indians of Arizona. The stimulation of 5-HT2C receptors has been shown to decrease food consumption, and is the target of the popular prescription appetite suppressant sibutramine (Meridia®). Meridia stimulates 5-HT2C receptors by blocking the reuptake of norepinephrine and serotonin, the major ligands for this adrenergic receptor.
See also: Drug Targets that Decrease Food Intake/Appetite; Pima Indians; Sibutramine (Meridia), Type 2 Diabetes.
Bibliography
L. Campield, et al., “Strategies and Potential Molecular Targets for Obesity Treatment,” Science (v.280/5368, 1998); S. H. Stahl, Essential Psychopharmacology (Cambridge University Press, 2000); 1996; A. D. Strosberg, “Association of Beta3-Adrenoceptor Polymorphism with Obesity and Diabetes: Current Status” Trends in Pharmacological Sciences (v.18/12, 1997).

{kind=link}