Dolores Price – A case study in Cyclothymic Disorder
I have been diagnosed with cyclothymia. Does that mean a quicker recovery?
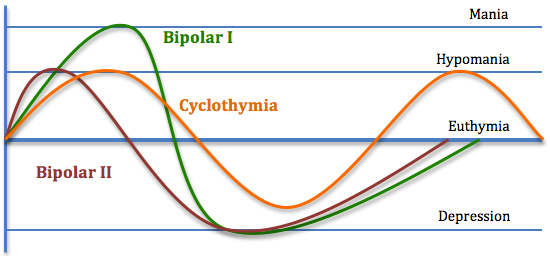
Cyclothymia is a more chronic, less severe form of bipolar disorder. By chronicity, it is meant that the mood states (either depression or hypomania) are more sustained than in bipolar disorder.
By severity, it is meant that the mood states are generally not associated with either vegetative symptoms (such as sleep, appetite, or energy disturbances) or psychotic symptoms (such as delusions of guilt or grandiosity). Cyclothymia is defined in the DSM-IVTR as having over a period of two years or more (one year in children and adolescents) the presence of numerous hypomanic episodes and numerous depressive episodes that do not meet the criteria for major depressive disorder.
It is the characteristic of the depressive episodes that differentiates cyclothymic disorder from bipolar II disorder (which does have major depressive episodes). Additional criteria include not having the absence of such symptoms for greater than a two-month period. Interestingly, both cyclothymia and bipolar II can be diagnosed if a major depressive episode occurs after the initial two-year period of illness. As with all illnesses, the symptoms cannot be due to substance use and must cause clinically significant distress or impairment in social, occupational, or other important areas of functioning. While cyclothymia is a distinct diagnosis, it is also considered one of the bipolar variants or spectrum disorders as described by Hagop Akiskal, a prominent research psychiatrist who outlined the variants in Psychiatric Clinics of North America. Akiskal’s schema of bipolar subtypes includes the following:
• Bipolar I: full-blown mania
• Bipolar I 1⁄2: depression with protracted hypomania
• Bipolar II: depression with hypomanic episodes
• Bipolar II 1⁄2: cyclothymic disorder
• Bipolar III: hypomania due to antidepressant drugs
• Bipolar III 1⁄2: hypomania and/or depression associated with substance use
• Bipolar IV: depression associated with hyperthymic temperament
These subtypes are increasingly receiving attention from clinicians because the concept of the bipolar spectrum is now capturing a range of behaviors typically classified under other conditions. As one can readily see, because the symptoms are considered less severe but more chronic than in bipolar disorder, the issue of quicker recovery becomes more complicated.
The first question to be considered is what treatment approach to take. Depending upon the level of distress or disability you are experiencing, the illness may warrant pharmacological intervention. The use of medications in the management of cyclothymia has not been researched however, mainly because the pharmaceutical companies that perform the majority of drug studies focus on the more severe forms of illness because it is easier to measure outcomes in response to medication. Thus any medication trial for cyclothymia or any bipolar variant will be largely empirical-that is, trial and error.
Second, because the symptoms tend to last longer than in bipolar disorder, psychotherapy is critical whether or not you choose pharmacological management because it will help you develop skills to deal more effectively with stressors in the environment and negative self-thoughts that may accompany mood swings. Many people suffering from cyclothymia have co morbid personality disorders, which respond better to psychosocial interventions than pharmacotherapy.
Terms:
Pharmacological – pertaining to all chemicals that, when ingested, cause a physiological process to occur in the body.
Psychopharmocological – refers to those physiological processes that have direct psychological effects.
Response – referring to at least a 50% reduction but not complete cessation of all symptoms associated with a specific mental illness, such as depression.
Psychosocial – pertaining to environmental circumstances that can impact one’s psychological well-being.




{kind=link}