HIV Replication 3D Medical Animation
Can I get HIV now that I am older?
Over 10% of all new AIDS cases in the United States occur in people over the age of 50 years. New AIDS cases in the past several years rose faster in middle age and older people than in people less than 40 years old.
Although many of these AIDS cases are the result of HIV infection at a younger age, many are due to becoming infected after age 50. Because very few persons over the age of 50 at risk for HIV routinely get tested, it is difficult to determine rates of HIV infection among older adults. Older adults are often first diagnosed with HIV at a late stage of infection when they seek treatment for an HIV-related illness.
HIV cases among older people may be underreported because HIV symptoms and infections may coincide with other age related diseases and are therefore overlooked. Fatigue, weight loss, and other early HIV symptoms may be dismissed as a normal part of aging. AIDS-related dementia is often misdiagnosed as Alzheimer’s disease.
Many characteristics of HIV are specific for older persons. Older individuals with AIDS get sick and die sooner than younger persons because of a late diagnosis as well as co infection with other diseases that may speed the progression of AIDS. In addition, new drugs for HIV treatment may interact with medications the older person is taking to treat preexisting chronic conditions.
A common stereotype exists in the United States: Older people don’t have sex or use drugs. Few HIV-prevention efforts are aimed at people older than 50 years, and most educational ad campaigns rarely show older adults, making them an invisible at-risk population. Older people, therefore, are generally less knowledgeable about HIV/AIDS than younger people and are less aware of how to protect them against infection. This lack of awareness is especially true for older injecting drug users, who comprise over 16% of AIDS cases in persons older than 50 years. Men who have sex with men form the largest group of AIDS cases among adults older than 50 years. Older gay men tend to be “invisible” and ignored both in the gay community and in prevention efforts. The HIV risk factors for older gay men include internalized homophobia, denial of risk, alcohol and other substance use, and anonymous sexual encounters.
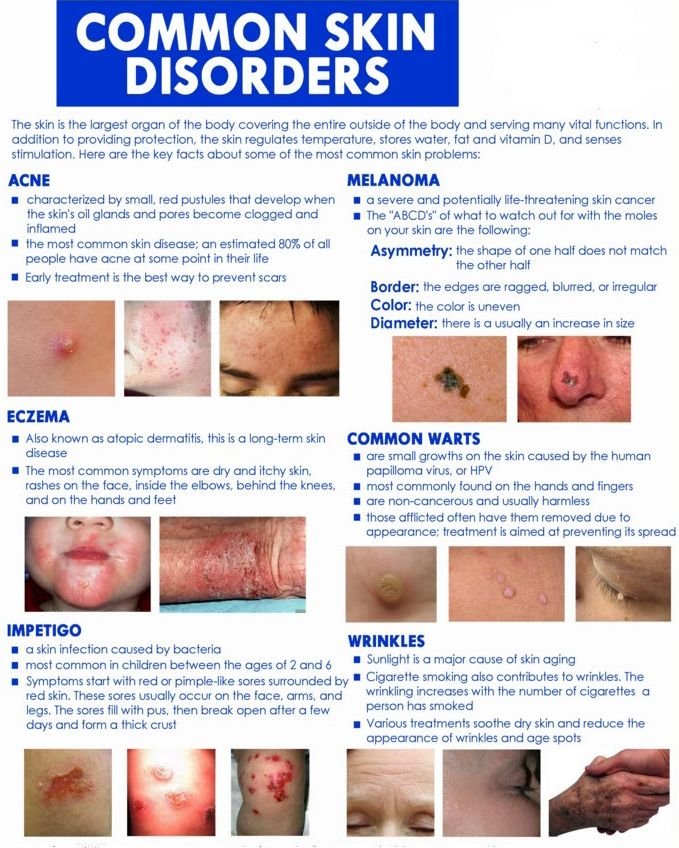
Skin lesions occur in virtually all patients during the unfolding evolution of their HIV infection-usually a succession of conditions reflecting the gradual decline of immunity. A transient rash may accompany the initial HIV seroconversion illness but may go unnoticed. During the following weeks or years, the gradually declining immunity may be documented only by decreasing numbers of CD4-positive lymphocytes with the emergence of inflammatory skin conditions (e.g., seborrheic dermatitis or psoriasis), as well as autoimmune conditions (e.g., thrombocytopenia, morphea, or alopecia areata).
As immunity itself declines, skin infections emerge. Shingles affects over 25% of HIV-positive patients and may be followed by postherpetic neuralgia. Molluscum contagiosum, warts, and dry skin may appear. In severe cases, the person may develop purplish nodules on the face and extremities and other locations, which are Kaposi’s sarcomas, a form of skin cancer.
Practice safe sex and use precautions!
Term:
Lesion – A vague term meaning “the thing that is wrong with the patient.” A lesion may be a tumor or an area of inflammation.
Shingles – An extremely painful rash that is caused by a viral infection known as herpes zoster.



{kind=link}