Obesity and Mortality
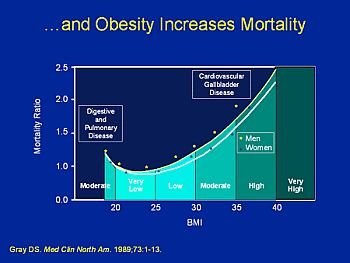
Majority of epidemiologic studies, mortality begins to increase with BMIs above 25 kg/m2. The increase in mortality generally tends to be modest until a BMI of 30 kg/m2 is reached.
For persons with a BMI of 30 kg/m2 or above, mortality rates from all causes, and especially from cardiovascular disease, are generally increased by 50 to 100 percent above that of persons with BMIs in the range of 20 to 25 kg/m2. Three aspects of the association between obesity and mortality remain unresolved:
Association of Body Mass Index with Mortality
Many of the observational epidemiologic studies of BMI and mortality have reported a ‘U-’ or ‘J-shaped’ relationship between BMI and mortality. Mortality rates are elevated in persons with low BMI (usually below 20) as well as in persons with high BMI. In some studies, adjustment for factors that potentially confound the relationship between BMI and mortality, such as smoking status and pre-existing illness, tends to reduce the upturn in mortality rate at low BMI, but in a meta-analysis the higher mortality at low BMIs was not eliminated after adjustment for confounding factors. It is unclear whether the elevated mortality observed at low BMI is due to an artifact of incomplete control for confounding factors, inadequate body fat and/or inadequate body protein stores that result from unintentional weight loss, or individual genetic factors.
Currently, there is no evidence that intentional weight gain in persons with low BMIs will lead to a reduction in mortality.
Association of Body Mass Index with Mortality in Older Adults
Many of the observational epidemiologic studies suggest that the relationship between BMI and mortality weakens with increasing age, especially among persons aged 75 and above. Sever factors have been proposed to explain this observation. Older adults are more likely than younger adults to have diseases that both increase mortality and cause weight loss leading to lower body weight. In addition, as people age, they tend to have larger waist circumferences that increase their risk of mortality even at lower BMIs. Also, weight in middle age is positively related to risk of mortality in old age. The impact of smoking on body weight and mortality is likely to be much stronger in older adults because of the cumulative health effects of smoking.
BMI, which is an indirect estimate of adiposity, may underestimate adiposity in older adults whose BMI is similar to younger adults. It is also possible that persons most sensitive to the adverse health effects of obesity are more likely to have died before reaching older ages, resulting in older cohorts that are more “resistant” to the health effects of obesity. Recently, a 20-year prospective study of a nationally representative
sample of U.S. adults aged 55 to 74 years suggested that lowest mortality occurs in the BMI range of 25 to 30. After adjusting for smoking status and pre-existing illness, lowest mortality occurred at a BMI of 24.5 in white men, 26.5 in white women, 27.0 in black men, and 29.8 in black women.
Association of Body Mass Index with Mortality in Ethnic Minorities
The levels of BMI associated with increased mortality are based on epidemiological studies of primarily white populations. The interest in confirming the association between BMI and mortality in other racial/ethnic groups stems partly from observations that lower-than-average total mortality has been observed among some populations with a high BMI level, and partly from observations that within certain populations there appears to be no effect of obesity at all or at the BMI levels that are associated with higher mortality in whites.
African-Americans:
Three small cohort studies of narrowly defined populations of African-Americans failed to show the expected association of BMI and mortality based on data from white populations. Although the shape of the association of BMI and mortality in two large, representative U.S. data sets (the National Health and Nutrition Examination Follow-up Study and the National Health Interview Survey) is similar for black and white males and females, the BMI-related increase in risk begins at a 1 to 3 kg/m2 higher BMI level for blacks than for whites. For example, in the National Health and Nutrition Examination Follow-up Survey, the estimated BMI associated with minimum mortality was 27.1 for black men and 26.8 for black women, compared with 24.8 and 24.3, respectively, for white men and women. On the basis of these data, the use of the cut point of BMI ³ 30 kg/m2 for defining obesity is clearly applicable to African-Americans as well as to whites.
Other Ethnic Minority Populations:
Limited data relating obesity to mortality in American Indians were identified, but no data were found relating obesity to mortality in Hispanic-Americans, Asian-Americans, or Pacific Islanders. The lowest mortality rate among Pima men is observed at a BMI range of 35 to 40 kg/m2 for men, and no relationship between BMI and mortality is observed among Pima women. Based on mortality data alone, it would be hard to justify using the same standard for defining obesity in populations, such as American Indians, among whom the mean BMI is much higher than in the general U.S. population.
However, diabetes-related morbidity among obese American Indians is extremely high, and the overall age-specific mortality among American Indians is generally higher than in the U.S. general population. Thus, obesity in American Indians is associated with a compromised overall survival of the population.
Although the data on mortality are still fragmentary for many minority populations, there are no studies that would support the exclusion of any racial/ethnic group from the current definitions of obesity. Secular trends in many populations in the United States and throughout the world have demonstrated that longstanding overweight and obesity eventually leads to the emergence of chronic diseases. Therefore, prevalent overweight and obesity cannot be ignored even where the associated health problems have not reached the level that would be expected on the basis of data for white populations.

{kind=link}