Diagnosis and evaluation
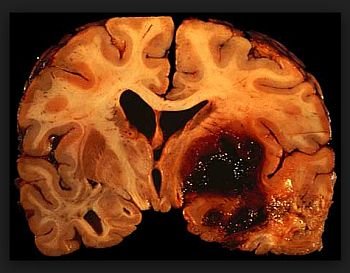
Intracerebral hemorrhage (ICH)
(Doctor only)
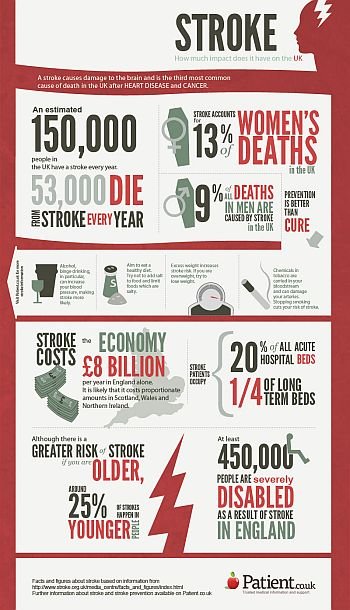
Stroke affects 0, 2% of the entire population, and more than 1% of people older than 65% years, each year. Stroke is fatal in up to one-third of cases, making it the third most common cause of death in developed countries, after coronary heart disease and cancer.
Among survivors of stroke, who comprises at least 0,8% of the general population, at least half are permanently disabled, making stroke a major cause of long-term physical cognitive, emotional, social and vocational disability.
As with ischemic stroke, management in the first few hours may make the difference between a good and bad outcome.
I N I T I A L ASSESSMENT
.History and physical exam.
Look for signs of trauma.
. Glasgow coma scale (GCS) and brainstem reflexes if comatose, NIHSS score if awake.
. Measure blood pressure (see subsequent comment for details on blood-pressure management).
. Oxygen saturation.
Consider intubation for airway protection.
. CT.
Repeat CT if patient was transferred from outside hospital (the bleed could have extended en route).
Where did the bleed start?
Is there significant mass effect, intraventricular hemorrhage (IVH), or hydrocephalus?
. Measure the volume (diameter Ax diameter Bx C)/2.
C = number of slices that show hemorrhage[1]thickness of the slice.
. Check platelet count, INR, and PTT, and urine drug screen.
. EKG: rule out MI.
Consider cardiac enzymes.
. Consider vascular study (MRA, CTA, or DSA) to rule out AVM or aneurysm.
Especially if:
. Younger patient; or
. There is SAH present; or
. ICH in an atypical lobar or cortical location, or with some other atypical appearance.
. Consider MRI:
To look for multiple old hemorrhages or microbleeds that might suggest amyloid angiopathy.
To exclude underlying tumor.
To check for venous thrombosis (order MR venogram if suspected):
. Hemorrhages high in convexity, often bilateral, with Substantial edema.
. Consider getting neurosurgery consult.
For possible hematoma evacuation or ventriculostomy;
If aneurysm or AVM suspected.
MANAGEMENT
It is important to talk with family and start the process of coming to terms with the often poor prognosis. This is a very important management consideration. Discuss ‘‘Do Not Resuscitate’’ (DNR) issues. However, in the first day, don’t be too certain of bad outcome unless herniation has already occurred. Comatose patients can wake up, especially if the mass effect is decompressed spontaneously into the ventricle, or by surgical intervention. Do not withdraw support in the ED.
SURGICAL INTERVENTION
. Surgical evacuation of hematoma is to prevent death from mass effect.
There is no evidence that routine surgical clot evacuation results in improved outcome (ISTICH trial).
. Surgical clot evacuation is usually reserved for patients with the following:
Younger age: no absolute cutoff but almost certainly<75 years.
Cerebellar hemorrhages with:
. Displacement of fourth ventricle;
. Enlargement of temporal horns (early obstructive hydrocephalus);
. Compression of brainstem;
. Decreased level of consciousness (but don’t wait until the patient is comatose if above criteria are met).
Supratentorial hemorrhages with:
. Superficial location: close to brain surface;
. Volume>20 cc;
. Drowsy but not comatose;
. More likely if not in eloquent location.
. Ventriculostomy and CSF drainage:
May be life-saving if obstructive hydrocephalus is present

{kind=link}