What Medications are Available to Treat BPH?
What are the results of BPH treatment using alpha-blocker drugs?
All six of the alpha blockers commonly used today in the United States have been demonstrated to be beneficial in the treatment of prostatic obstruction; however, both Phenoxybenzamine (Dibenzyline) and Prazosin (Minipress) are not commonly used anymore because to be effective they have to be taken more than once per day.
Terazosin (Hytrin) was studied in a randomized, placebo-controlled fashion and was found to be very effective in treating the symptoms of BPH. Two hundred eighty-five patients were entered into a study where placebo, or different doses of terazosin were given. Response rates were evaluated using subjectivemeasures (symptoms were improved) and objective measures (urinary flow rate).
The percentages of patients exhibiting a greater than 30% improvement in symptom scores and flow rates. Doxazosin (Cardura) has also been proven to be efficacious in the treatment of BPH. Five double-blind, placebo-controlled clinical studies of doxazosin have been published in the literature. These studies demonstrated that doxazosin improved objective measurements such as flow rates, as well as subjective measurements such as symptom scores.
Tamsulosin (Flomax) is a more selective alpha blocker than either terazosin or doxazosin. It therefore has alower systemic side-effect profile than terazosin or doxazosin. Like other alpha blockers, tamsulosin has a low incidence of dizziness (5.7%), hypotension (0.4%), or fainting (0.2%). Alpha blocker drugs have been proven effective in treating the symptoms that are often associated with an enlarged prostate. Whenever you gauge the effectiveness of any therapy for the treatment of prostate symptoms, it is important to have a control group, as there is often a significant placebo effect observed in the treatment of prostatism. It is important to recognize that symptom score improvement is a subjective measure based on the patient’s perception as to whether his symptoms have improved after taking a drug. The peak flow rate is an objective measure based on the force of the patient’s urinary stream measured by a machine. Alpha blockers have been shown to be efficacious in the treatment of obstructive prostate disease by both objective and subjective measures. To date, no study has yet shown that alpha blockers reduce the risk of going into urinary retention.
What is DHT?
DHT is a metabolite of testosterone that mediates secondary sexual characteristics, including prostate growth. The major male hormone, testosterone, is converted into DHT by an enzyme known as 5 alpha reductase. 5 alpha reductase was discovered independently in 1974 by Julianne Imperato-McGinley and Patrick Walsh. Julianne Imperato-McGinley was actually studying children in Santo Domingo with ambiguous genitalia and noted that when the male children grew up they never developed enlarged prostates. It was her work and that by PatrickWalsh that established that DHT was the active agent that mediated prostate growth.
Testosterone governs libido or sex drive and to some degree erectile functions. It controls the growth of the prostate indirectly as it is converted by 5 alpha reductase into DHT.
What types of 5 alpha reductase inhibitors are available?
The enzymes 5 alpha reductase are present in two isoforms: type 1 and type 2. Type 1 is found predominantly in extra prostatic tissues such as the skin and liver, although it is also found in the prostate. Type 2 is found predominantly in the prostate. Two drugs have been developed that inhibit 5 alpha reductase. The first is finasteride or Proscar, which is a type 2 or selective 5 alpha reductase inhibitor. The second is dutasteride or Avodart, which is a type 1 and type 2 or nonselective 5 alpha reductase inhibitor. Finasteride has been shown to reduce serum DHT levels by 70%, whereas dutasteride has been shown to reduce serum DHT by 90%. It is not yet known whether that difference in DHT suppression translates into greater efficacy for the patient.
Q. Because Proscar can cut a patient’s PSA levels by 50%, wouldn’t this also help to cut the patient’s risk of prostate cancer by 50%?
A: Currently, it is not known with certainty whether either finasteride or dutasteride can prevent the development of prostate cancer. Studies are ongoing to answer this question.
What are the side effects of 5 alpha reductase inhibitors?
Alpha receptors are found in tissues throughout the body; therefore, alpha blockers can cause side effects or symptoms not related to voiding. A variety of side effects have been reported with the use of alpha blockers for voiding dysfunction. These include dizziness, headache, postural hypotension, drowsiness, tachycardia (fast heart rate), skin rashes, dry mouth, diarrhea, nausea, vomiting, asthenia (weakness), chest pain, and erectile dysfunction. These side effects are rare, but the patient should discuss possible side effects fully with his doctor before starting an alpha blocker for voiding problems. In addition, alpha blockers can interact with some other drugs, particularly those used to treat high blood pressure, and these potential drug interactions should also be discussed with the treating physician.
Q. If a 5 alpha reductase inhibitor such as Proscar (finasteride) does block the conversion of testosterone into DHT and a patient taking Proscar finds his prostate continuing to grow, what other known substances might have a role in the growth of the prostate?
A. DHT appears to be the driving force causing prostatic growth; however, a variety of other growth factors may play a minor role as well.
What are the results of BPH treatment using 5 alpha reductase inhibitor drugs?
Finasteride (Proscar) and dutasteride (Avodart) are the two 5 alpha reductase inhibitors that are currently available in the United States. Both of these drugs require 3 to 6 months to see clinical beneficial effects. The Finasteride Study Group showed improvement in peak flow rates and symptom scores as well as a decrease in prostate volume.
At 1 year, patients on 5 milligrams of finasteride had a 22% improvement in peak flow rates and a 21% decrease in symptom scores. In addition, they exhibited a 19% decrease in their prostate volume. A recent report looking at cohort of patients treated with dutasteride showed similar improvement in urinary flow rates, a decrease in symptom scores, and a reduction in prostate volume.
What effects do 5 alpha reductase inhibitor drugs have on PSA levels?
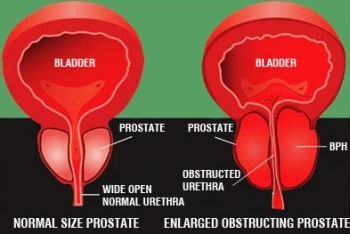
PSA is a valuable blood test that screens for prostate cancer, as discussed in Questions 5 to 11. However, 5 alpha reductase inhibitor drugs do affect PSA levels. 5 alpha reductase inhibitor drugs block the conversion of testosterone to DHT, which results in shrinkage of the prostate or a decrease in prostate volume. Because prostate cells make PSA, it is reasonable to assume that as the prostate gets smaller, the PSA level will decline. This is in fact what happens; however, it takes 3 to 6 months for a significantvolume decrease to occur and thus, the PSA decline is gradual. Nonetheless, by about 6 months after starting a 5 alpha reductase inhibitor, the total PSA level is about half of the baseline value. The free fraction of PSA is not changed by treatment with 5 alpha reductase inhibitors.
This influence of 5 alpha reductase inhibitors on PSA does not diminish the usefulness of PSA in managing patients with prostate disease. For example, if a 65-year-old man has been on a 5 alpha reductase inhibitor for 6 months, a PSA is drawn, and the value returns as 3.2 ng/ml with 22% free fraction; a simple doubling of the total value to 6.4 ng/ml is made, and the free fraction remains unchanged at 22%. The clinician and patient can then react to the 6.4, 22% value, as would be their custom with any other patient in that age range.

{kind=link}