High BP and planning a pregnancy
I have had high BP for several years and would now like to plan a pregnancy. What precautions should I take?
The most sensible approach for a woman with known high BP planning a pregnancy is to seek pre-pregnancy advice from a well-informed doctor physician or specialist obstetrician. General advice will include maintaining a sensible balanced diet and normal weight for your height, taking regular exercise, stopping smoking and either stopping alcohol or keeping intake to a minimum. All women who are planning a pregnancy are advised to take extra folic acid (a vitamin that plays an important part in the development of the fetus) for 3 months before a planned pregnancy (e.g. before you stop using contraceptives) and for the first 3 months of pregnancy. Specific advice will relate to whether your high BP requires treatment, what BP-lowering drugs are safe to use in pregnancy, whether you could stop your medication for the early part of pregnancy and whether there are additional risks to your health or that of your baby because of your high BP. It is highly unlikely that you will be advised not to have a pregnancy because of high BP.
We hear a lot about how drugs taken in pregnancy can damage unborn babies – I’m especially thinking of thalidomide, but I know there are others. Can BP-lowering drugs be safely taken in pregnancy?
The time when we are most concerned about drugs affecting the fetus (the unborn baby) is in early pregnancy. Your pregnancy begins before you miss your period, but for the first week when the fertilized egg is moving down your fallopian tube, it is probably not at risk from drugs in your bloodstream. The important time for development is from the time of implantation up until the end of the third month, a period known as ‘organogenesis’ because all of the baby’s organs and structures are developing. After the first 3 months of pregnancy the baby is mostly just growing and is much less vulnerable to any effects from drugs.
If you are taking BP-lowering drugs, then you should take the earliest opportunity to discuss with your doctor (or whoever else is looking after your BP) whether or not you need to change your type of drug or whether it would be safe for you to stop treatment. Ideally this will have been planned before your pregnancy as discussed in the previous question.
Ever since thalidomide (which, incidentally, was a sleeping tablet and was used for morning sickness – it was not a BP-lowering drug), all drugs have been tested on animals (mostly rabbits or rats) to see if they might cause organ damage to the fetus during pregnancy. Because very large numbers of animals can be used, these tests are fairly sensitive, but because they are not on humans, we can never be entirely sure that they exclude risks to a human fetus. New drugs are rarely tested in pregnant women and often not even in women of reproductive age. We have to rely on more indirect evidence from population based studies and on reporting of bad outcomes (adverse event reporting) where pregnant women have inadvertently taken drugs.
Thousands of women and babies have been checked in this way for evidence of fetal damage from drugs taken in pregnancy and, on the whole, these studies have been reassuring. None of the common BP-lowering drugs has been shown to produce fetal damage, although many women have conceived while taking their regular BP-lowering medication. Unfortunately this is not the same as proving safety. Although damage on the scale of thalidomide is certainly not happening, serious damage to as few as 1 baby in every 1000 born is possible. We have to take this risk seriously, while at the same time not being alarmist. Naturally there is greatest experience and reassurance about safety with the older BP-lowering drugs. For this reason, you may be advised to change from a newer type of BP-lowering drug to a more old-fashioned one when planning a pregnancy or when you are seen in the early stages of an unplanned pregnancy.
What does this mean in practice?
There are three things to consider.
• BP-lowering drugs should be avoided in pregnancy, unless your raised BP is serious enough to justify this.
• Plan your pregnancies with the help of a well informed doctor or obstetrician and, if you do need BP-lowering drugs, you can be confident that you will be prescribed the safest possible choice.
• Discuss the possibility of temporarily interrupting your treatment with BP-lowering drugs during the weeks when you are attempting to conceive and during the first 13 weeks of your pregnancy.
I have tried different BP-lowering drugs for my hypertension and they haven’t always suited me. What options will I have in pregnancy?
You will obviously want to avoid any drugs that could cause additional risk to you or to your baby. Methyldopa is an old-fashioned drug, which, although it does have some side effects, has a good track record for safety and effectiveness at all stages of pregnancy. Beta-blockers are well tolerated and apparently without risk to the baby after 24 weeks; before this they may slow down the baby’s growth and should be given only if necessary. There is most experience with labetalol, but atenolol should be avoided as this agent was implicated in a small study showing impaired growth in fetuses.
The calcium-channel blockers are commonly used in later pregnancy, but there is much less safety data than for methyldopa or beta-blockers and they are best avoided in early pregnancy unless there are reasons for not being prescribed other types.
Diuretics, often the first choice for high BP, are ruled out because they may make pre-eclampsia worse (pre-eclampsia is discussed later in this chapter). However, this risk is probably theoretical and many women will have taken diuretics in early pregnancy with little evidence of side effects to themselves or their babies. However, you will probably not be given them in pregnancy. The drugs that really need to be avoided for your baby’s sake are the ACE inhibitors, which have known dangers for the developing baby (usually later in pregnancy) and newer agents that are completely unevaluated in pregnancy.
High BP in pregnancy
I have heard that BP falls in pregnancy. Why is this?
Yes, it normally falls during pregnancy. This is one of the reasons why you may be able to stop BP-lowering drugs for at least part of your pregnancy. If it rises, this is always important, because it may indicate that you have pre-eclampsia or eclampsia. Nurses, doctors, and midwives regularly measure your BP all through pregnancy looking for newly elevated BP or the development of pre-eclampsia.
Pregnancy normally lasts between 38 and 42 weeks. This is usually divided into three periods of development, called trimesters. The first 13 weeks (the first trimester) roughly corresponds to the time when the baby is being formed. The second trimester is from 14 to 27 weeks: it used to be the time when the baby was thought to be too immature to survive, but now some babies as young as 24 weeks do survive with intensive neonatal care. Babies were considered able to survive if they were born during the third trimester (which runs from 28 weeks of pregnancy until the birth), although before modern intensive care many failed to do so.
From whatever level it starts, your BP normally falls during the second trimester (from 14 to 27 weeks). It then usually rises slowly until your baby is born (which is normally at 38 to 42 weeks), although it may still be a bit lower than before you became pregnant. After your baby is born your BP rises slowly over the first 5 days to regain its usual level before your pregnancy. When you are pregnant, not only do you need oxygen, but so does your developing baby. Your body therefore makes more blood to carry enough oxygen for both of you, so the total volume of your blood rises rapidly during the first 12 to 13 weeks of your pregnancy. All other things being equal, a rise in blood volume should cause a rise in BP. To prevent this, your placenta (which nourishes your baby in your womb, links your blood supply with your baby’s, and is expelled in the afterbirth following the birth of your baby) releases hormones (mainly progesterone), which relax the walls of your veins and small arteries so that they become larger to make room for this increased blood volume, without any rise in your BP. Because of this, your heart doesn’t have to pump so hard and your BP falls.
Because your blood vessels are relaxed, they do not respond as quickly to instructions from your brain, so blood may remain in your legs when you get up out of a chair. Your BP then falls, and you may feel dizzy or faint. All this usually happens in the first 12 weeks or so when your circulation is changing most rapidly, but even later in pregnancy you may find yourself feeling faint in a hot room or if you get up too quickly from lying down. If this happens you should either sit or lie down and it will usually pass off quite quickly.
When I’m pregnant, how high must my BP be to be called high BP?
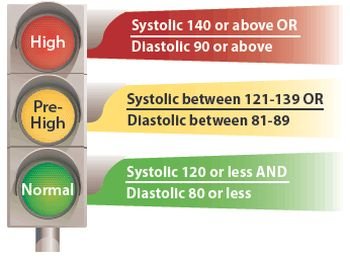
A BP of 140/90 mmHg or more is conventionally considered to be a high BP in pregnancy. The significance of these figures will depend on whether your high BP is new (i.e. developing for the first time in your pregnancy) or whether it was already high before you became pregnant.
Why is it important to know if my raised BP developed before I became pregnant or whether it is something new?
The difference between pregnancy in women with pre-existing high BP (i.e. having raised BP before you became pregnant) and high BP starting in pregnancy is simply the rate of change ofyour BP. Pre-existing high BP starts very slowly, in childhood or adolescence, with plenty of time for every part of your body to get used to it. High BP developing for the first time during pregnancy develops over a very short time, never more than a few weeks and occasionally even over a few hours. During this time you may get very serious damage to your small arteries, particularly in the kidneys, liver and brain. It may also affect the blood supply to the placenta and ultimately the oxygen supply to your unborn baby. The same kinds of damage may occur in preexisting high BP, but only at much higher levels of BP, and usually over much longer periods of time.
If I get high BP during my pregnancy, who should look after it, my doctor or my obstetrician?
If your BP rises for the first time during pregnancy, i.e. you didn’t have high BP before you were pregnant, then your obstetrician will take the decisions about your treatment, although your doctor and midwife also need to know what drugs (if any) you are taking. Because BP can change very quickly in pregnancy, your doctor or midwife should check your BP if at any time you feel ill, have pain in the upper part of your abdomen, or a prolonged headache. These are important warning signs of pre-eclampsia. Your antenatal clinic should give you your maternity notes so that you can show them to anyone you need to consult, although in some areas you may instead be given a card called a shared-care card on which all this information can be recorded. Don’t forget to take your notes with you whenever you go to the clinic or to see your doctor.
Not many women are both young enough to be pregnant and at the same time old enough to have BP high enough to need BP-lowering medication. This means that not many obstetricians see women with long-standing high BP who have already had treatment for months or years. However, this pattern is changing with more women delaying child bearing to an older age, and you may well have a choice of healthcare professionals who can offer care. If you are affected by high BP, then you need joint care, intelligently shared between your doctor or your hospital physician, your obstetrician and your midwife. Because your medication is likely to be changed during your pregnancy, you will need more frequent BP measurements than most women, and they will need to be very accurate.
I’m in my first pregnancy, and my BP has gone up a bit. My doctor says she’ll keep an eye on it but that I don’t need any drugs for it yet. If I do need to take BP-lowering drugs, when will I start on them?
Speaking generally, if BP rises for the first time after 36 weeks of pregnancy, then it is usually best to deliver the baby within a reasonable interval, so labour is brought on early (induced). This decision may be made without you needing BP-lowering drugs. If BP starts rising for the first time between 24 and 30 weeks, doctors usually try to control it with BP-lowering drugs so that the baby is more mature when born and has a better chance of surviving.
Between 30 and 36 weeks BP-lowering drugs may help to prolong the pregnancy and increase the likelihood of you being able to have a normal delivery and reduce the likelihood of the baby needing medical support in the intensive care unit.
Doctors vary in their opinions on how high your BP should be before you start treatment. There is good evidence that treatment benefits both mother and baby when systolic BP measures 170 mmHg or more or diastolic BP measures 110 mmHg or more. This level of high BP is an indication for admission to hospital and immediate stabilization on BP-lowering drugs. There is far greater variation in practice when BP is between 140/90 and
160/100, what is called mild to moderate hypertension. Some studies suggest that treatment of mild to moderate hypertension may reduce the chance of progression to severe hypertension; however, the counter argument is that there may be a negative effect on the growth of the baby. There is clearly a balance to be achieved in treating moderate hypertension in pregnancy between potential benefit and harm. You will need to discuss this with your obstetrician who can take account of your individual circumstances and what approach is likely to result in the best outcome for you and your baby.


{kind=link}