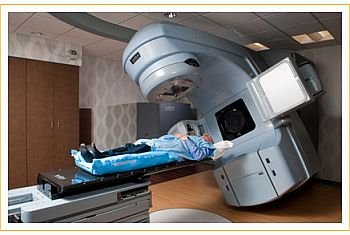
Radiation Therapy
Radiation therapy (RT) brings waves of energy particles into contact with cancer cells. It can be delivered by an external beam through a machine called a linear accelerator (the most common form of RT), directly implanted into a cancer in the form of radioactive seeds (called brachytherapy), administered intravenously (such as radioactive iodine given for thyroid cancer), or coupled to monoclonal antibodies (such as Bexxar and Zevalin used to treat lymphoma). RT is also used in other ways.
It is tempting to think of radiation therapy as zapping cancer cells much like a laser in Star Wars obliterates an enemy ship. In fact, though, patients receiving RT are told that an MRI or CT scan to assess the results of their treatment will not be performed for several weeks after the completion of RT in order to “give the treatment time to exert its full effect.” This is because radiation delivers an energy burst to cells, setting in motion a number of reactions that over time cause the cell to die. Just like the drug therapies discussed above, radiation can cause damage to DNA and interference with the signals communicated inside cancer cells; it can even exert an angiogenesis inhibitory effect by killing the endothelial cells that form blood vessels. The result is that RT causes cancer cells to undergo cell death.
To improve the results with radiation, researchers are studying the addition of targeted therapies to RT. One of the most impressive results was recently reported using Erbitux in combination with RT to treat head and neck cancer. The combination greatly increased survival compared to treatment with radiation alone. The addition of chemotherapy to this combination is being studied.
Why Do Cancer Treatments Sometimes Fail?
Drug resistance or the growth of cancer in the face of ongoing or recently completed treatments represents the main barrier to cure for many cancers. When a patient experiences a remission, his or her hopes for cure or prolonged cancer control are naturally raised. It is therefore upsetting and often disorienting to be told that the cancer has relapsed, that the treatments have suddenly stopped working.
In most instances, oncologists cannot specify why a person’s cancer develops treatment resistance. We rely on the discoveries of laboratory researchers, who themselves are busy sorting through the myriad of possible scientific reasons for resistance to just one particular drug. If this seems like a bit of double talk, it just might be; treatment resistance is probably the most complicated area of oncology. The root cause of a cancer relapse lies in the fact that cancer is not an accumulation of exactly the same cells but rather a mixture of cells with differing properties. Some may have sensitivity to certain drugs and be killed by them, whereas others are resistant to those drugs. The resistant population will survive treatment and in time be detected as a cancer relapse. For cancers that can be cured, the available therapies can match all that the cancer can offer by way of resistance. For those that cannot be eradicated, newer treatments are needed that overcome this resistance.
Drug resistance may be present in an untreated cancer or emerge in response to therapy. This property explains the acquisition of resistance during a cancer’s growth.
Chemotherapy may lose its effectiveness when cancer cells activate a protein that pumps the drugs out as soon as they enter the cells; targeted therapies may lose their ability to control their targets when those receptors and signaling proteins mutate and morph into different shapes; hormone therapies may stop controlling cancer growth when the estrogen or androgen receptors undergo a shape change or get massively overproduced, overwhelming the drugs meant to neutralize them. Through an understanding of the specific genes and proteins responsible for drug resistance, researchers are developing new chemotherapies, targeted therapies, and hormone treatments that may be effective when available treatments stop working.
Exciting new research is shedding light on the “natural” drug resistance of some cancers. Several types of cancer have been found to contain a very small population of cancer stem cells, which are believed to be responsible for continually replenishing the pool of cells in a tumor.
It turns out that an additional property of these cancer stem cells is their natural resistance to chemotherapy and other cancer treatments.
If the molecules driving the growth of these cells could be specifically targeted by drugs, the treatment of many cancers may improve. The first reported payoff of this approach was presented at the 2008 meeting of the American Association for Cancer Research (www.aacr.org). The study involved patients with aggressive basal cell skin cancer treated with a pill (named GDC-0449) that targets a molecule called “hedgehog.” Of the first nine patients enrolled in the study, eight experienced shrinkage or no further growth of their cancer. Targeting cancer stem cells will undoubtedly be an important avenue of research in the years to come.
Breast and prostate cancers depend on the hormones estrogen and testosterone to make them grow. Hormone therapies decrease the levels of hormones, resulting in cancer death.




{kind=link}