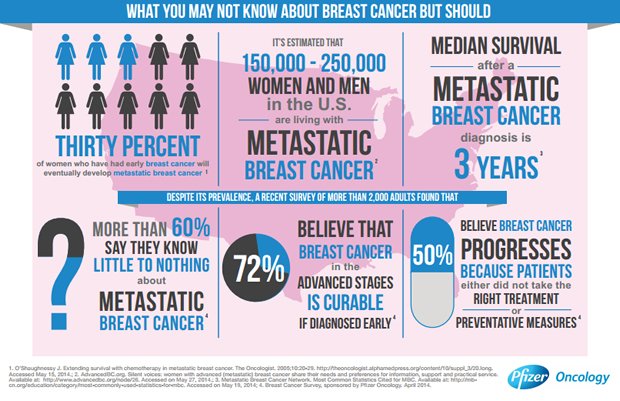
The untold story of the advanced or metastatic breast cancer patient
I have osteoporosis. Is it safe to take an aromatase inhibitor?
Although AIs (anastrozole, letrozole, exemestane) are usually the hormonal treatments of choice in postmenopausal women with metastatic breast cancer, they may cause problems for women with osteoporosis. The effect of the AIs on bones is well recognized. They tend to worsen bone loss and increase fracture risk, but simply having osteoporosis does not mean that a woman cannot use an AI. Rather, these women do need to have their osteoporosis managed aggressively and followed closely.
All women should have a bone density study (DEXA scan) before starting an AI. If you are not already doing so, you should take appropriate calcium and vitamin D3 supplements. If you have been taking these supplements regularly, and your bone density scan shows significant osteopenia or osteoporosis, you should start taking oral bisphosphonates, such as alendronate sodium (Fosamax), risedronate sodium (Actonel), or ibandronate sodium (Boniva). If you have only osteopenia and have not been taking calcium and vitamin D3, it is reasonable to try these supplements first. By following your bone density on repeated DEXA scans, your doctor can see if these oral therapies are working. Most insurance companies will pay for only one DEXA scan a year; this is usually adequate in this situation.
If these measures do not work, intravenous bisphosphonates, such as zoledronic acid (Zometa) given two to three times per year, may allow you to remain on an AI. On the other hand, if you have no major risk factors like blood clots, you and your doctor may want to consider switching to tamoxifen. It is still an excellent drug for breast cancer and it has less risk of aggravating your osteoporosis. If you are prone to falling or have already had a broken bone due to osteoporosis, you should probably simply avoid the AIs altogether.
Term:
Osteopenia – A condition of less bone density or bone mass than would be normally expected if you compare a woman to a woman or population of women her age. It is the bone loss that, if it continues, can lead to osteoporosis.
I am taking hormonal therapy for treatment of my metastatic breast cancer. Is it true that chemotherapy is better than hormonal therapy since it is given intravenously?
No; hormonal therapy is usually given by mouth and it has fewer side effects than most intravenous chemotherapies. Many cancer patients make the mistake of thinking that medicine given in the veins is more powerful than medicine given by mouth. This is not true. It does not really matter how the anti-cancer medicine gets into your body, as long as it does. Some medicines are not absorbed into the bloodstream through the gastrointestinal tract, so doctors have to administer it directly into the bloodstream through a vein. Another common misconception about cancer therapy is to assume that the severity of its side effects is directly related to its anti-tumor strength. Just because a treatment is toxic does not mean that it is effective, and the lack of toxicity does not correlate with inactivity. Unfortunately, many cancer treatments are associated with debilitating side effects, but their anti-cancer effect relates to how the cancer cells respond to the drug, not how it affects your normal cells. Hormonal therapy can actually be more effective than intravenous chemotherapy in a woman whose tumor expresses hormone (estrogen or progesterone) receptors, especially when her metastatic disease is confined to the bones or soft tissue.
Many cancer patients make the mistake of thinking that medicine given in the veins is more powerful than medicine given by mouth.
What kind of side effects might I expect to experience as a result of getting treatment for my metastatic breast cancer?
There are various side effects that a patient may experience while receiving treatment for metastatic disease as well as symptoms of progression of disease that warrant discussion with your doctor. Some are easily controlled and some may be more difficult. No two patients are alike so don’t assume if you knew someone with metastatic disease in the past that your situation will mirror theirs. You should discuss these with your oncology team so you know what to expect in relationship to the status of your metastatic disease and the treatment recommendations they are making on your behalf. These questions are not intended to alarm you but to provide you with a comprehensive list of possible issues that may need to be addressed while undergoing treatment.
Marissa’s comments:
The side effects from chemo and hormonal therapy were really getting to me. My most miserable problem was night sweats that prevented me from sleeping well. I found that installing a ceiling fan above my bed and keeping it on low all night really helped. Wearing cotton short sleeve and sleeveless nightgowns instead of pajamas that were long sleeved with long pants has been a godsend too. I even found a thing called a “chillow pillow” online that keeps my head feeling cool all night. This makes dealing with these symptoms from treatment a lot more tolerable and doable long term now Jill’s comments:
I attended a support group provided by the hospital where I’m receiving my treatments. It is for breast cancer survivors but most of the women who were attending were diagnosed early and were completing treatment or had finished treatment long ago. They were fussing and moaning about their hair growing back slowly, or having hot flashes still. This group was not for me and I told the social worker who was the facilitator so.
I finally found a group that was specifically for women with metastatic breast cancer. We are all in the same situation— some with disease that is very advanced and others with disease that is more stable but the bottom line is we share the same worries, fears, and hopes. I can relate to these women.

{kind=link}