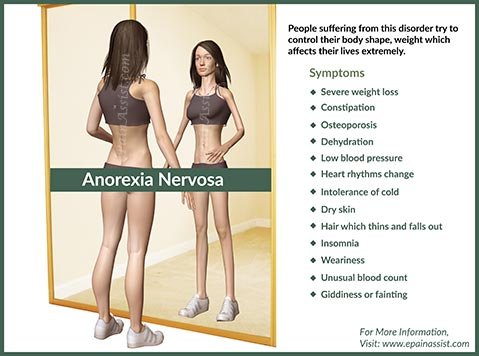
Anorexia Nervosa: Being Too Thin – An Inside Story BBC DOCUMENTARY
What effect does anorexia have on relationships?
Anorexia nervosa is an isolating illness. The mood and personality changes that result from semi-starvation can wreak havoc on close personal relationships and family ties. To begin with, the symptoms of anorexia demand a great deal of focus and attention: calorie counting, meal planning, exercise, purging behaviors, preoccupation with weight, and scrutinizing of one’s own appearance and body image. All of these require energy, which is already a limited commodity for the person in a semi-starved state. Thus, anorexia patients often gradually restrict their activities and narrow their interests to those having to do with food restriction, exercise, and necessary work or schoolwork.
Anorexia can take its toll on close relationships. For many loved ones, feelings of powerlessness, frustration, and resentment can build, increasing strain and inadvertently furthering the pattern of patient isolation and withdrawal. Fear and discomfort at the sight of an emaciated loved one can make for understandably tense interactions. Indeed, some recoil out of a paralyzing uncertainty about “what to say” (e.g., “Should I tell her that she looks frail?” “Do I treat her as though there is nothing wrong?”). Irritability and moodiness, constant fighting over meals, tense outings at the supermarket, desperate attempts to get a loved one to eat; all of these patterns can result in guilt, anxiety, worry, resentment, and anger, emotions that can strain family and marital relationships. Sadly, anorexia has been known to destroy the connectedness that was once shared in otherwise loving families.
Relationship problems may be further compounded in social gatherings that center on food due to the enormous pressure anorexia patients experience in such situations. Some patients will eat socially but only to keep up appearances while they simultaneously experience an overwhelming urge to restrict.
Others face frantic feelings of anxiety and are distracted by the need to purge or compensate for calories ingested. Social discomfort is further exacerbated when there is co-occurring social phobia, a social anxiety disorder often found in anorexia patients. Such individuals may desire interpersonal connectedness but avoid social situations due to intense fear or anxiety. Two related disorders that frequently co-occur in patients with anorexia are avoidant personality disorder (AVPD) and dependent personality disorder (DPD). In AVPD, people display pervasive and long-standing traits of shyness, social withdrawal, stranger anxiety, and fearfulness in social situations. Individuals with AVPD generally have a negative self-evaluation, feel socially “incompetent,” and are therefore quite reluctant to become involved in activities that require social interaction. An estimated 15–25% of eating disorder patients with a co-occurring personality disorder are diagnosed with AVPD. In contrast, patients with DPD are described as “extreme people pleasers.” These individuals tend to intensely fear separation from others, excessively seek reassurance or caretaking from loved ones, and have difficulty asserting their own opinions or desires. Individuals with DPD are often terrified of losing approval or support; therefore, they are often reluctant to disagree with others. Anorexia patients who are already prone to self-doubt and self-criticism belittle their own abilities to an even greater degree when DPD is present.
I was entrenched in my eating disorder throughout my teen and young adult years, which is the time that most people go through puberty and learn much about successful relationships. I always believed I had no problems with relationships. In one way it was
true, because I didn’t have any real relationships. I was focused almost entirely on the eating disorder for a couple of decades. After achieving some recovery, I struggled in my first job because I didn’t have good relationship skills. I was one of the hardest working and dedicated employees, but I never let anyone know who I was. Most people are very uncomfortable with this. It was a team environment, and I didn’t know how to be a team member. I couldn’t be invisible any longer. I finally understood how the many years in the eating disorder had kept me from learning basic social interactions, especially those derived from a real sense of self-confidence, which is vital for survival in the business world.
Sarah shares:
My eating disorder consumed every moment of every day and became the only steady relationship in my life. It prevented me from ever keeping a boyfriend or making new friends, and after a while, even my closest friends gave up on me. I distinctly remember one time when my two best friends came over to my house simply to tell me, “We give up. We just can’t do this anymore, Sarah.” That was when I completely lost hope. If even my best friends didn’t believe I could overcome my anorexia, how could I believe in myself?
At the worst of it, everything I did was dictated by a voice inside my head that made me feel like the only means of being in control of my life were running more, eating less, and essentially destroying my body. In reality, it was quite the opposite: The more I let my anorexia control me, the less control I had over my life.
Diagnostic Indicators for Avoidant Personality Disorder (AVPD)
AVPD is defined as a pervasive pattern of social inhibition, marked by feelings of inadequacy and hypersensitivity to negative evaluation, beginning by early adulthood and present in a variety of contexts, as indicated by four (or more) of the following:
• Avoids occupational activities that involve significant interpersonal contact because of fears of criticism, disapproval, or rejection.
• Is unwilling to get involved with people unless certain of being liked.
• Shows restraint within intimate relationships because of the fear of being shamed or ridiculed.
• Is preoccupied with being criticized or rejected in social situations.
• Is inhibited in new interpersonal situations because of feelings of inadequacy.
• Views self as socially inept, personally unappealing, or inferior to others.
• Is unusually reluctant to take personal risks or to engage in any new activities because they may prove embarrassing.
SOURCE: American Psychiatric Association. (1994). Diagnostic and statistical manual of mental disorders, 4th ed., Text Revision (p. 721).
Diagnostic Indicators for Dependent Personality Disorder (DPD)
DPD is defined as a pervasive and excessive need to be taken care of that leads to submissive, clinging behavior and fears of separation, beginning by early adulthood and present in a variety of contexts. A partial list of associated behaviors may include:
• Difficulty making everyday decisions without an excessive amount of advice and reassurance from others.
• Need for others to assume responsibility for most major areas of his or her life.
• Difficulty expressing disagreement with others because of fear of loss of support or approval.
• Difficulty initiating projects or doing things on one’s own.
• Going to excessive lengths to obtain nurturance and support from others.
• Feeling uncomfortable or helpless when alone and urgently seeking another relationship as a source of support when a close relationship ends.
• Unrealistic fears of being left to take care of himself or herself.
SOURCE: American Psychiatric Association. (1994). Diagnostic and statistical manual of mental disorders, 4th ed., Text Revision (p. 721).

{kind=link}