Cognitive Behavior Therapy for Substance Abuse
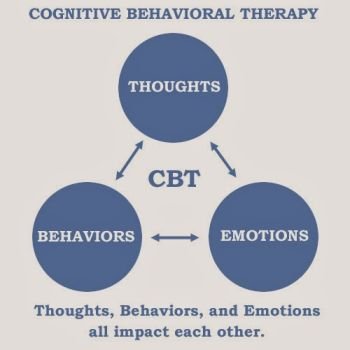
What is Cognitive Behavior Therapy?
Cognitive Behavior Therapy uses cognitive and behavioral interventions in changing faulty cognitions, which hinder cessation of drug use and improving skills.
Social skills training address the following:
1. Consequential thinking to identify the antecedents and consequences of substance use behavior
2. Self-control in resisting impulse to use substances and peer pressure and to develop drug refusal skills
3. Avoiding trouble by identifying and avoiding high-risk situations for substance use and associated problem behaviors
4. Social networking by identifying prosocial activities and new, nonsubstance-using friends
5. Coping with authority by using negotiation and compliance skills
6. Problem solving for effective and prosocial solutions in difficult situations
7. Relapse coping by developing strategies for dealing with subsequent substance use behavior
What is Relapse Prevention?
Relapse Prevention is a cognitive behavioral approach aimed at developing self-control; identifying triggers in the environment leading to use and relapse; and developing coping skills in dealing with stressors, triggers, and lapses into substance use.
The individualized Relapse Prevention plan incorporates family responsibilities in supporting the child’s sobriety.
What is a harm-reduction approach?
Harm reduction is a comprehensive philosophy used to decrease the negative effects of drug use on society. It presupposes that a society has to deal with the presence of drug use because it can never be totally eradicated. Some may even see harm reduction as the end of or a means to abstinence and by no means should be viewed as a tool of drug legalization.
Principles of harm reduction have been applied in situations that have generated responses ranging from endorsement to protest and controversy. Harm reduction approaches include the Methadone Maintenance Treatment Program’s aim at decreasing opioid use, delinquency, criminality and health problems; exchange needle programs to decrease HIV transmission; decriminalization of cannabis use in certain states and countries like the Netherlands to address illicit use and its legal consequences; and education and outreach on opioid overdose preventions.
Does harm reduction make drug use acceptable?
It would seem so, but only temporarily. Harm reduction can be seen as a means to the goal of full abstinence. If adolescents can achieve one goal at a time, starting with a decrease in drug use, then a decrease rather than cessation itself will be a step to the goal. This approach will allow adolescents to set realistic goals that they are able to achieve with concrete results.
What is Motivational Enhancement Therapy?
Motivational Enhancement Therapy (MET) as a means to further engage adolescents in treatment and retain them. MET is aprinciples of motivational psychology, that is designed to produce rapid change whose underlying motivation comes from within the individual. Rather than being therapist driven, motivational strategies are used to facilitate an individual’s own change. Motivational Enhancement Therapy arose from practical issues raised by clinicians in dealing with substance use, especially with people who are reluctant or ambivalent to change. Strategies are persuasive rather than coercive. It creates dissonance that is conducive to change. The overall goal is to increase intrinsic motivation.
Five general principles are:
1. Express empathy as the adolescents do not see any problem with using
2. Develop discrepancy; present the pros and cons of drug use and tilt the arguments against use
3. Avoid argumentation- avoid direct confrontation and challenges
4. Roll with resistance, accepting the current level of resistance to treatment and lack of motivation thereof
5. Support self- efficacy; the adolescent will have the final say to make the change
I am opposed to medications. When should I consider medication for my child?
Very frequently, parents express opposition to medication in general. There is limited success in the use of medication to affect abstinence. This is especially the case when dealing with adolescents. In addition, most studies are based on adults. Even fewer case studies mentioned the use of medications to decrease craving. Medications are clearly helpful in treating symptoms of withdrawal from certain drugs like alcohol, opioids, and benzodiazepines, and use of methadone or buprenorphine (Suboxone) is helpful as a detoxification medication or for maintenance. Medications can also be very helpful if drug use is also co morbid with moderate to severe depression, anxiety, psychosis, and ADHD. In fact, to resist aggressively treating these co morbid conditions can result in continued drug use. These conditions have to be treated aggressively and concurrently, and the adolescent will likely need a combination of treatments (medications and psychotherapy) on a long term.
Physicians make use of medications for the following reasons:
1. To treat comorbid psychiatric disorders (stimulants for ADHD)
2. To take advantage of drug- aversive agents (like disulfiram for alcoholism)
3. To treat withdrawal effects (methadone for heroin or opioids)
4. To block reinforcing effect of drugs (buprenorphine for opioids)
5. To substitute a similar drug for prolonged maintenance (methadone for opioids)
6. To treat craving (modafinil for cocaine)
Substitution therapies and aversive agents are infrequently used in adolescents. However, if these medications can increase the likelihood of treatment success or at least prevent further problems, parents should discuss these options with the physician. Parents are hesitant about considering medications to treat substance abuse without coexisting psychiatric conditions in their children. While studies are limited, use of medications to treat substance abuse without coexisting psychiatric worked and have few side effects. Bupropion (Wellbutrin) has been used for adolescent nicotine addiction, ADHD, and depression. Buprenorphine (with or without naltrexone [Subutex or Suboxone]) has been studied and found to be safe and effective for adolescents who abuse opioids. Other medications that have been used and studied include medications that decrease craving for alcohol like disulfiram (Antabuse), naltrexone (Revia), acamprosate (Campral), and topiramate (Topamax), a medication used for seizures and bipolar disorder.
There are experimental drugs that are currently being investigated, including rimonabant and ondansetron for marijuana abuse.
Edith’s comments:
I see that my son really needs his bipolar medication. John goes through ups and downs and he would smoke weed to bring himself down. He also experimented with cocaine.
With Lithium, his mood became stable and he stopped using. Hopefully, it will be longer this time.
Terms:
Cognitive behavior Therapy – Therapy that uses cognitive and behavioral interventions to improve skills and change maladaptive behaviors, which hinder cessation of drug use.
Relapse Prevention – A cognitive behavioral treatment approach aimed at developing self-control; identifying triggers in the environment leading to use and relapse; and developing coping skills in dealing with stressors, triggers, and lapses into substance use.
Harm-reduction approach – Treatment approach that consists of strategies in minimizing the impact of alcohol use and other high-risk behaviors. It operates on the theory that abstinence and minimal harm are goals, but proponents also recognize that any behavior changes that reduce harm are, by themselves, positive outcomes.
Motivational Enhancement Therapy – A type of evidence based, non-coercive, and self-centered psychotherapy aimed at increasing the likelihood to change behaviors. As it applies to addiction. Motivational Enhancement Therapy increases the imbalance toward accepting the need to change from drug-seeking to nonusing behaviors



{kind=link}