AMERICAN PSYCHOLOGICAL ASSOCIATION
AMERICAN PSYCHIATRIC ASSOCIATION
There is a fascination about psychiatry that goes beyond the natural curiosity about how the body or mind works. Psychoanalysts have suggested that this fascination (often mixed with fear) is because mental illnesses act out our own inner dramas. We see the depression we are struggling with and containing displayed before us, or individuals losing control when we may fear or secretly long to let go and shed our inhibitions. There is certainly some truth in this. Psychiatry is, like all medicine, a pragmatic problem-solving
activity. It draws on scientific theories but is not derived from them or constrained by them. Unlike psychology or physics, psychiatry cannot be explained ‘top-down’ from theories. Psychiatry has been formed by the illnesses that it has been required (and agreed) to treat and further shaped by the treatments it had available at the time. The development of psychiatry is dependent on the values and structures of the societies that fostered it. It is almost impossible to understand current practices without understanding some of that history. I have devoted so much space to the controversial aspects of psychiatry for two reasons. First, because there are real philosophical and ethical differences between mental and physical illnesses that won’t go away simply because we want them to. Nor will technological advances obliterate these tensions; The challenge for psychiatry in the 21st century may be particularly acute in ethical and social questions posed by increasingly sophisticated and powerful treatments of the mind.
Secondly, psychiatry is the arena where many of the big questions of the time – philosophical, political, and social – have to be hammered out in the crucible of real human relations and suffering. The philosophical debate about free will and determinism comes alive in the courtroom arguments about a psychiatric defence or in policy decisions about the management of psychopaths. The politics of power and social control drove the dismantling of the asylums and now frames the debate on compulsory treatment. The mind–brain dichotomy hovers throughout. The sustained battering from the anti-psychiatrists in the 1960s and 1970s raised the right (indeed, they would say the existential obligation) to be different.
So welcome to an area of medicine that is both mysterious and exciting as advances in brain sciences continually bump up against the messy reality of human beings. It is an activity which despite the scanners and designer drugs still rests on establishing trusting personal relationships. And lastly welcome to a pursuit that keeps challenging us about what it is to be truly human; continually reminding us of those unresolved philosophical issues (free will, mind–body dualism, personal autonomy versus social obligations) that we usually push to the back of our minds in order to get on with life.
What is psychiatry?
The only normal people are the ones you don’t know very well. All of us know someone who has been troubled (anxious, depressed, or confused). Most of us have felt that way ourselves sometimes (adolescence is often a particular time of self-doubt and unhappiness). At these times our emotions may be overwhelming, unpredictable, and impossible to control and our thoughts strange and bizarre.
Does this mean that we have been mentally ill or need to see a psychiatrist? Luckily the answer for most of us is no. Yet when we read about psychiatry what we find described are experiences remarkably similar to these. Psychiatry is fascinating because it deals with consciousness, choice, motivation, free will, and relationships – indeed everything that makes us human. While it is often cloaked in forbidding jargon (‘affect’ instead of mood, ‘anxiety’ instead of worry, ‘phobia’ rather than fear, ‘cognition’ instead of thinking) the conditions described are still instantly recognizable.
This is one of the persisting paradoxes about psychiatry that will recur throughout this book – that its subject is simultaneously firmly rooted in common human experience and yet is somehow ‘that bit different’. We recognize similar experiences to our own in what the patient describes. They are immediately familiar to us, yet these familiar experiences are used to diagnose disorders quite outside our experience. Hopefully by the end of this book you will understand this dilemma better but I can’t promise to resolve it for you. It’s been argued about since psychiatry came into being and the argument still goes on. However, it may be best to start by defining what psychiatry is (and what it is not) before returning to the philosophical and political controversies that attend it.
All the ‘psychs’: psychology, psychotherapy, psychoanalysis, and psychiatry ‘Psyche’ is the Greek word for mind. All these four terms describe different approaches to understanding and helping individuals with psychological and emotional (mental) problems. There is lots of overlap, and sometimes the work done by the same highly qualified individual can be described by several of these terms, so it is not surprising that people confuse them. However, there are differences and getting them clear will help clarify what psychiatry is.
Psychology
Psychology is the study of human thought and behaviour. It originated just over a century ago from a tradition of introspective philosophy (trying to understand the minds of others by understanding our own) and is now a firmly established science. Psychology is studied at school and as an undergraduate course at university. It encompasses the study and understanding of mental processes in all their aspects and it has many branches. Experimental psychologists conduct experiments to explore the very basics of mental functioning (perception, memory, arousal, risk-taking, etc.). Indeed experimental psychologists do not restrict themselves exclusively to humans but study animals both in their own right and as models to understand human behaviour.
Experimental psychology is generally considered a ‘hard science’ which follows the same scientific principles of investigation as physics or chemistry. There are several professions stemming from psychology (e.g. educational psychologists, industrial psychologists, forensic psychologists). Clinical psychologists have postgraduate training in abnormal psychology and use this understanding to help people deal with their problems. The most obvious early example of this approach was the application of learning theory (i.e. consistent rewards and punishments to shape behaviour) in behaviour therapy. Behaviour therapy has been particularly successful in helping disturbed children or those with learning difficulties to modify their behaviour. It works without requiring a detailed understanding of the issues by the patient. Psychological treatments have, of course, become much more sophisticated and currently one of the most successful and widely practised psychotherapies (cognitive behaviour therapy) has been developed by clinical psychologists and is provided mainly by them. Clinical psychologists are essential members of all modern mental health (‘psychiatric’) services.
Psychoanalysis
Psychoanalysis is the method of treating neurotic disorders developed by Sigmund Freud towards the end of the 19th century in Vienna. In psychoanalysis the patient is encouraged to relax and say the first thing that comes into their mind (‘free association’) and to pay attention to their dreams and to the irrational aspects of their thinking. Freud was convinced that his patients suffered because they tried to keep unconscious (repress) thoughts and feelings that were unacceptable to them and that doing so caused their neurotic symptoms. The analyst listens carefully to what is said and over time begins to detect patterns and clues to these ‘conflicts’. By sharing these insights he helps the patient confront and resolve them. Psychoanalysis is intensive and very long with patients
traditionally coming for an hour a day up to five times a week for several years. Psychoanalysis is the origin of the cartoon image of the bearded psychiatrist sitting behind the patient lying on the couch. Although Freud was a doctor there is no requirement for psychoanalysts to be medically trained. In America (where psychoanalysis has always had its most powerful presence) analysts were usually also psychiatrists but this is now increasingly the exception. Even when medically trained, analysts rarely use their medical knowledge – they make a virtue of not ‘interfering’ beyond the analysis. There are several schools of psychoanalysis developed by disciples of Freud (e.g. Jung, Adler, Klein) and some have become quite remote from the original model (e.g. Reich, Lacan). Psychoanalysis has had enormous influence beyond psychiatry, particularly in literature and the arts. Terms like ‘Freudian’ and ‘Freudian slip’ are part of everyday speech.
However, because psychoanalysis lacks firm scientific evidence of its efficacy, it is increasingly marginalized in modern psychiatric practice.
Psychotherapy
It soon became clear that there was more to psychoanalysis than Freud’s original remote and neutral exploration of the unconscious. The relationships formed in this intense treatment were themselves found to be influential. Analysts began to explore these relationships and experimented with more active approaches and with different types of therapy (time-limited therapies, more structured therapies, therapies in groups and in families, etc.). These psychological approaches, in which the relationship was used actively through talking to promote self-awareness and change, are broadly understood as ‘psychotherapy’. Most of the early psychotherapies leant heavily on Freud’s theories (often called ‘psychodynamic psychotherapy’ to emphasize the impact of thoughts and feelings over time) but several of the newer ones do not. These (e.g. non-directive counselling, existential psychotherapy, transactional analysis, cognitive analytical and cognitive behaviour therapy) draw on a range of theoretical backgrounds.
What they all have in common is that they use communication within a formalized and secure relationship to explore difficulties and find ways of either adapting to them or overcoming them. Most psychodynamic psychotherapies also require (like psychoanalysis) that the therapist undergoes a treatment themselves as part of the training. Psychoanalysis remains very tightly controlled, by defining strictly who becomes a psychoanalyst, but psychotherapy is a loose concept. Some schools of psychotherapy are strict about whom they admit but the title ‘psychotherapist’ could, until recently, be used by anyone. Most psychotherapists are not psychiatrists although most psychiatrists have some psychotherapy training and skills. Some psychiatrists even work mainly as psychotherapists.
So if it is not psychology and not psychoanalysis or psychotherapy, what is psychiatry? There are overlaps with the other ‘psychs’ but there are some fundamental differences. First and foremost psychiatry is a branch of medicine – you can’t become a psychiatrist without first qualifying as a doctor. Having qualified, the future psychiatrist spends several years in further training. He or she works with, and learns about, mental illnesses in exactly the same way that a dermatologist would train by treating patients with skin disorders or an obstetrician by delivering babies. Within medicine, psychiatry is simply defined as that branch which deals with ‘mental illnesses’ (nowadays often called ‘psychiatric disorders’).
Medicine is fundamentally a pragmatic endeavour. While drawing heavily on the basic biological sciences and scientific methods, the ultimate test of whether a treatment is right is if the patient gets better. We don’t have to know how the treatment works. Therefore the definition of psychiatry is not based on theory, as in psychology or psychoanalysis, but on practice. Whatever is viewed as mental illnesses (and this has changed over time), and whatever treatments are available for these illnesses, will determine what a psychiatrist is, and what he or she does.
What is a mental illness?
There is a marked circularity about this (‘a psychiatrist is someone who diagnoses and treats psychiatric disorders’, ‘psychiatric disorders are those conditions which are diagnosed and treated by psychiatrists’). There has been endless controversy about the reliability of psychiatric diagnoses and even whether or not mental illnesses exist at all. It is worth spending a little time on why psychiatric diagnoses are so controversial both because it keeps cropping up and also because the same issues are fundamental to all medicine although rarely as striking.
The subjectivity of diagnosis
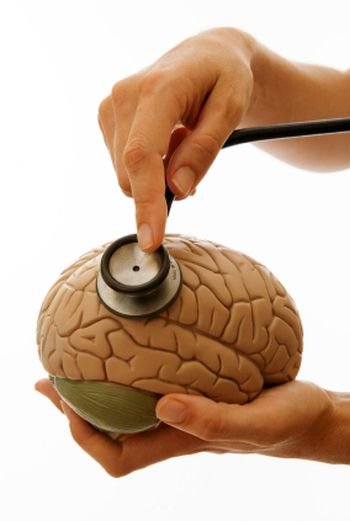
The hallmark of the psychiatrist’s trade is the interview. We make our diagnoses (and still conduct much of our treatment) in face-to-face discussions with patients. We take a careful history (as do all doctors) but then, instead of, or sometimes in addition to, conducting a physical examination (feeling the abdomen, taking the pulse, listening through a stethoscope) we conduct what is called a ‘mental state exam’. In this we probe deeper into what is worrying the patient, their mood, way of thinking, etc. Some of this involves simply noting what the patient reports (that they are hearing strange sounds or that they panic every time they think of going out) but some involves us in constructing an understanding of what they are going through using ‘directed empathy’. Directed empathy means actively putting ourselves in their shoes, understanding what they are feeling and thinking, even if they have difficulty in expressing it. For instance we may come to the conclusion that a patient who recounts a series of vindictive acts carried out against them by strangers and friends alike is, in fact, excessively suspicious (paranoid) leading to misinterpretation of common events.
This ability to piece together how other people experience things and what they are feeling is an essential human capacity. Understanding how others see the world from their perspective (often called having ‘a theory of mind’) is so important that its absence, as in Autism or Asperger’s Syndrome, is a profound handicap. Psychiatrists train up this skill and, because of increasing familiarity with the range of disorders, can use it actively to understand the confused and confusing experiences that patients recount to them.
Diagnoses based on a patient’s mental state contain no concrete evidence for the diagnosis – there are no blood tests or x-ray pictures.
A written list of what is said or a detailed description of the behaviour (e.g. the diagnostic criteria for depression) are only part of the process. Psychiatric diagnoses rely on making a judgement about why someone is doing something, not just the observation of what they are doing. Hence the criticism that they are not scientific; they are not ‘objective’. Take the example of an elderly man who is profoundly depressed. He may not say that he is depressed but instead complain of tiredness, aches and pains, poor sleep and feelings of guilt. As he deteriorates he may lie unmoving all day or even not speak at all.
A psychiatrist will probably interpret his immobility as a feature of depression. In doing this (usually supported by the other clues) he hypothesizes that the immobility is a result of despair and hopelessness. There are lots of other possible causes of immobility (or ‘stupor’ in its most extreme form) and the psychiatrist distinguishes depressive stupor from those caused by hormonal or neurological problems by building up a picture of the patient’s mental state, i.e. why he is not moving or communicating.


{kind=link}