Ebola Caused More Freak Outs Than Outbreaks In 2014 (VIDEO)
Ebola: Mapping the outbreak (BBC)
2014 – The Year Ebola Challenged the Humanity
EBOLA-2014-World Health Organization
Poliomyelitis – World Health Organization
Observational and experimental studies
The principles of epidemiology hitherto outlined apply to all studies, although the examples and the discussion have focused on observational studies, in which the investigator intervenes only by observing people and recording information at a point in time or during a time period. The great advantage of this type of study is that it can in principle be carried out in all contexts to investigate any health phenomenon. The disadvantage is that all comparisons between rates and risks in different groups of people, for example rates of chronic bronchitis among those exposed to air pollutants in a city and those not exposed, can always be influenced by unknown factors other than the pollutants. The elaborate procedures outlined in the previous chapters are necessary in these observational situations to reach conclusions about the possible causal role of an exposure such as air pollution on a disease such as chronic bronchitis.
Life would be simpler if the epidemiologist could choose, as in a laboratory experiment, which subjects would be assigned polluted and unpolluted air to breathe for several years, making sure in advance that all subjects in the experiment were closely similar in all respects, except for the `treatment’, i.e. exposure to different types of air. The simplest and safest device to achieve this similarity would consist in assigning the subjects perfectly at random, by tossing a coin, to breathing polluted or unpolluted air.
The random assignment would act as an insurance against all known and, crucially important, unknown factors that could make the two groups of people different. Clearly this randomized experiment, or randomized controlled trial (RCT), is not feasible, both for ethical and technical reasons. Hence the lesser scope of experimental randomized studies (also generically and less accurately called `intervention studies’) in respect to observational studies, notably when an agent, like polluted air, is investigated because of possible adverse effects on health. The elective place of the randomized experiment is in investigating agents which may have beneficial health effects. Promising new drugs are continuously tested on population of patients affected by a great range of diseases, from all kinds of cancer to heart diseases like myocardial infarction and angina pectoris to rheumatic diseases. In addition to these trials of treatment, large randomized experiments are carried out in healthy populations to test preventive interventions. Screening programmes for early diagnosis and treatment of serious conditions such as breast or colon cancer are tested in population randomized experiments and new vaccines – for example, against AIDS – are commonly tested using randomized trials in large populations.
The first vaccine against poliomyelitis
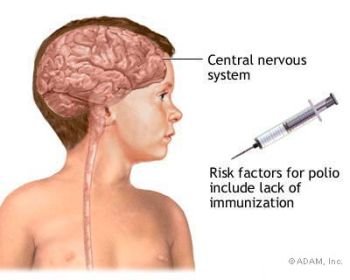
Until the middle of the last century, poliomyelitis, or infantile paralysis, was an infectious disease of the nervous system occurring especially in summer in epidemic waves, irregular in intensity. It affected particularly children and young people, who might experience only a transient fever or instead suffer lifelong flaccid paralysis of the limbs, or die if the nervous centres controlling respiration were attacked by the virus causing the disease.
Three types of the virus had been identified. Some small-scale but unsuccessful attempts with vaccines had been made when, in the early 1950s, a very promising vaccine to be administered by intra-muscular injection was developed by Dr Jonas Salk at the University of Pittsburgh. It consisted of a `killed’ virus that had lost its ability to produce the disease while retaining the power to stimulate a protective immunity in the body of the vaccinated subjects.
Before recommending the vaccine for mass administration, sound evidence of its actual efficacy was needed. Just starting to administer the vaccine and seeing whether the incidence rate was declining was not an option as the disease frequency varied too much from one year to the next. It would have been impossible to distinguish a decrease due to the vaccine from spontaneous variation. An additional problem was the difficulty in correctly diagnosing as poliomyelitis, rather than for example `flu’, the numerous minor cases which were the main source of the spread by direct contact between people. The decision was then taken to implement a true prevention experiment on primary school children.
Children aged 6 to 9, whose parents had agreed to take part in the study, had to be assigned at random to receive the vaccine or a no-vaccine treatment. They were recruited in 84 counties of 11 states across the whole territory of United States. The number of participants had to be very large, so that even if the vaccine gave only a 50% protection, a difference in the incidence rate between the vaccinated and the unvaccinated group would be detectable with a high degree of confidence. One dose of the vaccine against all three types of the virus had to be administered at the start of the study, a second dose one week later, and a third after five weeks. The no-vaccine treatment consisted of three injections but of an inactive preparation strictly similar in appearance to the vaccine, i.e. a placebo. When feasible, placebo treatments are the best form of comparison for an active medication as it is well established that simply receiving an inactive medication may produce an effect. One may wonder, however, whether ethics committees would today approve injecting children three times with an inactive preparation. The trial was `double blinded’ as not only the children (and their families) did not know whether they were receiving the vaccine or the inactive preparation, but their physicians were also unaware of which treatment was administered. In this way, they would not be influenced at all by knowledge of the treatment when, confronted with a suspect case, they would have to decide about a diagnosis of poliomyelitis.
Close to 400,000 children whose parents had given consent were entered into the trial (200,745 vaccinated and 201,229 unvaccinated) out of a total of about 750,000 in the areas where the trial took place. 82 cases of poliomyelitis were observed among the vaccinated children in the six months after vaccination, i.e. a risk of 41 per 100,000 and almost double, 162 cases, were observed among the unvaccinated, a risk of 81 per 100,000. The difference between the two risks, 81-41 = 40 is larger than would be expected by chance if there was no real difference. An even stronger decrease was noted for the more serious form (paralytic) of the disease, with risks of 16 per 100,000 in the vaccinated group and 57 per 100,000 in the non-vaccinated. The conclusion here is much more straightforward than in the case of an observational study. Because the children were assigned at random to vaccination and no-vaccination, the two groups should be closely similar in all respects except for the difference in treatment, which can be confidently regarded as the cause of the decreased rate among the vaccinated children. The trial demonstrated the effectiveness of the vaccine and initiated programmes of systematic vaccination all over the world.
The Salk vaccine is even today considered to be the most effective and safe protection against poliomyelitis. Five key features of randomized controlled trials. The study design is always based on randomization, usually implemented today by means of computer-generated lists of random numbers. People can just be assigned at random to the different treatments or some additional condition can be introduced. For instance, in a trial of nicotine patches for smoking cessation, subjects were randomly assigned to different types of patches or to a placebo within each centre participating in the study. In this way, correct comparisons of treatments became possible not only overall on the pooled data from all centres but also within each of the centres located in different countries.
The choice of the study population is critical for generalizing the conclusions drawn from a trial. In the nicotine patches experiment, volunteer subjects were recruited who had made two or more previous unsuccessful attempts and who were going to receive advice by a physician. The conclusion of the trial, that the patches effectively increase the probability of stopping smoking, would not necessary apply to less motivated people. Moreover, treatments that have been shown to be effective and safe in adults may not work in the same way in old people or children. As a general principle, a treatment (e.g. a drug) for a specific disease should be prescribed only in subjects closely similar to those in the trials that have demonstrated its efficacy.
The incessant pressure from the pharmaceutical industry to extend the use of a drug to other diseases should be resisted until there is clear evidence that it works for them as well. To be informative, a trial should include a sufficient number of subjects. What a ‘sufficient’ number is can be calculated at the planning stage based on the size of the difference between treatments one wishes to detect with a high degree of confidence. If one is interested in picking up only a very large effect, for example the complete elimination of a disease by a vaccine, a relatively small number will be adequate because if such a major effect exists, it is likely to show up in any event. If at the opposite end one wishes to show that a new vaccine that is cheaper and easier to administer is not (or only minimally) different in efficacy from the best vaccine hitherto available, a very large number of subjects will be required to exclude the possibility that the new vaccine is not inferior, even by a small but still statistically significant amount, to the old one.
The treatment can be as simple as a drug or a vaccine or much more complex, such as an intervention to modify the habitual diet. A recent randomized trial in this field showed that a reduction in the intake of calories could reduce weight in volunteer subjects keeping their amount of physical activity nearly constant. Remarkably, it also showed that the composition of the diet did not matter, whether high or low (within reasonable limits) in fat, protein, or sugars, provided the diet was low in caloric content. Keeping to the diet within the trial implied, however, repeated contact and strict surveillance of the subjects, something that may not be easily reproduced in the population.
Basically, a randomized trial is justified when there is genuine uncertainty about the effect of a treatment in respect to a placebo or to another already established treatment. This uncertainty materializes a condition of `equipoise’ between the treatments.
Usually several responses to the treatment or endpoints will be assessed to measure the intended and the possible adverse effects of the treatment. The incidence rate of myocardial infarction may be measured in a trial testing a drug aimed at its prevention but any other anomalous manifestation will also be carefully monitored as it may indicate an adverse effect of the drug. The best device to avoid all conscious and unconscious influences on the observation and recording of the endpoints is to keep both subjects and physicians blind to the treatments administered. This may not always be possible as, for example, when the treatments are diets of different compositions.
The analysis of the data collected during the study is done at the planned end of it. Often, however, some intermediate analyses can be done to monitor what is happening: if early indications of an obvious advantage of one of the treatments emerge, it may become unethical to continue with the other and inferior treatments; or if signs of serious adverse effects show up, it may become necessary to stop the trial. Because of these delicate implications, the intermediate analyses are usually placed in the hands of a trial-monitoring committee independent of the investigators responsible for the study. A particular type of analysis is not infrequently necessary to take into account the fact that a proportion of trial participants will abandon their assigned treatment during the course of the trial. Most likely these dropouts do not occur by chance but because, for instance, some subjects find it too cumbersome to adhere to a diet, or simply dislike it. In these circumstances, a comparison of the effects of different diets on, for example, the incidence rates of diabetes between people who kept to their diet throughout the trial would not reflect the reality. A more realistic analysis, named by intention to treat, will compare the diabetes rates between the groups of people as initially assigned to each diet, regardless of whether some people dropped out in each group. In fact, the net effect of a diet as it may be proposed, if beneficial, to the whole population will be the result from the combination of the effects among those who adhere to it and whatever other effect ensues among those who started it but then switched to other regimes.
Randomized, non-randomized, and spontaneous experiments Randomized trials are a precious tool in medical and epidemiological research. They can be looked at from two slightly different angles. From one viewpoint, they are the instrument to test how effective a treatment is. Before the era of the randomized control trial, heralded by the British trial of streptomycin on pulmonary tuberculosis in 1948, the evidence of the positive and negative effects of a treatment was essentially based on the accumulation of clinical experience supported by knowledge from physiology and pathology.
In epidemiology the evidence of how, for instance, a vaccine worked was based on observational studies. Compared to randomized trials, these methods are more cumbersome, as they require a large accumulation of concordant results from clinical or epidemiological observations before any sound conclusions can be drawn, and less sensitive, because minor but medically important effects – say, a 5-10% reduction in the incidence rate of a disease – cannot be recognized with any confidence. The randomized trial has therefore become the generally accepted standard for testing treatments, preventive or remedial.
From another angle, the randomized trial is the acid test of causality. Removal of a presumed cause of a disease conducted in the form of a randomized trial is the best proof that the exposure is indeed a cause. This test may sometimes be feasible. For example, a vaccination programme against the hepatitis B virus could not be introduced all at once in the whole population of newborns in the Gambia. This unfavourable circumstance was turned into an actual advantage by picking the children to be vaccinated first at random, so allowing a correct comparison with the unvaccinated children born in the same year (by the fourth year, the vaccination reached all newborns in the country). The expected reduction in liver cancer among the vaccinated children once they become adult should provide conclusive evidence that the hepatitis B virus causes not only hepatitis – an established fact – but liver cancer, the most frequent cancer in many countries of Africa and South East Asia. For many exposures clearly indicated to be harmful by observational studies and laboratory experiments, a planned randomized removal of the exposure is neither feasible nor ethical. A surveillance programme should nonetheless be set up to observe the course of disease following the `natural experiment’ of removing (in whatever way) the exposure. For instance, a substantial number of the doctors in the prospective study of Richard Doll and Austin Bradford Hill stopped smoking. Already within the first five years after stopping, the incidence rate of lung cancer fell by almost one-third, providing additional and strong evidence supporting the causal role of tobacco smoking.
When overall survival is examined, the experience of British doctors showed that the sooner smoking is stopped the more an (ex)smoker can expect to live as long as a lifelong non-smoker. In plain terms, the best option is to never start smoking, the next best is to stop soon, and even stopping late produces at least some rapid benefit. Well-designed, conducted, and analysed observational and randomized.Studies are two complementary instruments of epidemiology that contribute to advancing knowledge even when they produce contrasting results, as the case of vegetables and cancer shows. Thirty years ago, several observational studies had already indicated that the consumption of vegetables, a source of vitamin A, and blood levels of vitamin A higher than average were associated with a reduced risk of cancer. T
here was some evidence from laboratory experiments showing that vitamin A and its derived compounds in the body could inhibit the transformation and proliferation of normal cells into cancer cells. To test directly the causal hypothesis that vitamin A inhibits cancer, a randomized controlled trial was carried out on more than 8,000 adult smokers (particularly at risk of lung cancer) in Finland comparing a placebo treatment with the administration of beta-carotene, the precursor substance of vitamin A present in yellow vegetables and fruits. The results turned out to be opposite to the hopes. The trial had to be stopped because a surge of lung cancer showed up in the men receiving the beta-carotene. This could mean that beta-carotene given at the doses of the trial, appreciably higher than in a normal diet, had an adverse rather than a beneficial effect. It might also mean that in the previous observational studies, vitamin A was not responsible for the reduced risk of cancer but simply an indicator of other substances present in vegetables and capable of inhibiting cancer development. Even today, the protective role of vegetables appears plausible, though not conclusively demonstrated, while on the other hand, the beta-carotene example gives a clear warning that incautious use of vitamin supplements may result in harmful rather than beneficial health effects.

{kind=link}