Facts about Sudden Cardiac Arrest (Video)
Cardiac Arrest – American Heart Association – When Minutes Count
What is cardiac arrest?
Cardiac arrest is the stopping of any heart pumping action. Naturally, that means that all blood circulation to the entire body stops as well. Cardiac arrest is by no means any particular heart rhythm diagnosis. The underlying arrhythmia that most commonly causes cardiac arrest is ventricular fibrillation, especially in those who experience acute heart attacks. Occasionally, the lack of any electrical activity at all in the heart can cause cardiac arrest. In addition, the disorder may be due to other extremely slow and ineffective heart rhythms.
From a clinical standpoint, cardiac arrest usually occurs together with pulmonary arrest (absence of lung function, which prevents effective breathing). This combination can lead to what you’ve heard described as cardiopulmonary arrest (the absence of both heart and lung function at the same time). As in cases of ventricular fibrillation, emergency treatment for cardiac or cardiopulmonary arrest (e.g., CPR, electrical cardio version, and the like) is essential.
What are the general guidelines for heart attack management?
Patient comment:
When you feel as though you are having a heart attack, you should stop all of physical activity at once and lie or sit down. You or a person nearby-a friend or family member, or even a passing stranger with a cell phone if necessary- should call 911 for immediate medical attention; it is important that you get to the nearest hospital emergency room quickly.
However, you should never drive your own car-that’s far more dangerous than simply waiting for the ambulance, because if you become unconscious, you could wind up in an accident, possibly killing yourself and maybe even someone else. Even when you are not sure whether you are having a heart attack, if you know you have high risk for heart attacks, it’s better to over-diagnose (or overreact) than to respond too late to the real thing. Do not hesitate to call the EMERGENCY even if you wonder whether it is only a false alarm.
Immediate cardiopulmonary resuscitation (CPR) and direct-current shock (defibrillation) are essential for your survival of sudden cardiac death. As soon as a heart attack occurs, either you or your family members or friends should dial the emergency number to request an ambulance. The emergency number dispatcher will contact the emergency medical services (EMS) system. When the emergency number system is not available, you or others should contact the emergency medical response system in the local area. The EMS responders should reach you within 4 to 5 minutes. As time permits, you or others acting for you should also inform your family (private) physician.
If you are conscious, you should chew one regular strength aspirin-chew it, don’t just swallow it, because chewing it will speed up its absorption. Studies have shown that taking aspirin while an acute heart attack is in progress can reduce the death rate by 25%.
Aspirin is effective in inhibiting blood clotting, so taking it improves and maintains blood flow through a narrowed heart artery, which can make the difference between life and death in some patients.
You should stop all physical actions and situate yourself, or have others situate you, in the most comfortable body position (lying or sitting). You could take nitroglycerin (up to three tablets) under your tongue if it has been prescribed before for angina. Do not take someone else’s nitroglycerin on the assumption that it will help-it might make matters worse! If you were found unconscious, as soon as is possible any family member or friend trained in administering CPR-and certainly the responding paramedical personnel-should initiate CPR. As you are being transported by an ambulance to a nearby hospital emergency room (ER), those in the EMS team will provide this emergency treatment as needed until you are stable. They should also give you any available emergency cardiac drugs promptly as needed. And, of course, continuous medical care will be provided in the ER. Do not try to deny what is happening in such circumstances; avoiding the truth can literally be fatal to heart attack victims. And you should avoid self-diagnosis or self-treatment (this is especially true for someone who might be a physician). It goes without saying that you shouldn’t be driving in this condition; again, don’t try to get yourself to the hospital, call an ambulance instead.
Early diagnosis followed by effective early medical care is extremely important for a better chance of survival and a good outcome. As soon as you are examined in the ER and undergo necessary diagnostic tests, the most important treatment is thrombolytic therapy (the use of special mediations that dissolve blood clots). These agents will reperfuse (i.e., restore circulation) in the damaged heart muscle. .
The management of acute heart attack is carried out primarily by five major modalities as follows:
• Various medications
• Electrical shock treatment (defibrillation) and artificial pacemaker
• Coronary angioplasty (percutaneous transluminal coronary angioplasty or PTCA.
• Coronary artery bypass graft (CABG)
• Cardiopulmonary resuscitation (CPR)
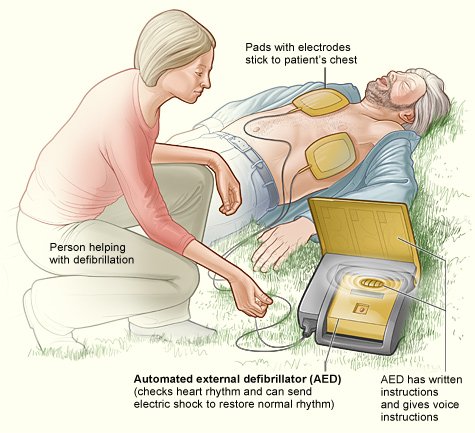
For ventricular fibrillation (chaotic, irregular and ineffective rapid heart rhythm arising from the ventricles), electric shock should be applied immediately using automatic external defibrillators (AEDs). Otherwise, sudden death cannot be prevented in most cases. Most ambulance teams carry portable defibrillators, and many police and fire rescue units are also equipped with defibrillators.
AEDs are very simple to operate and are also available in some commercial airplanes and public places (e.g., large sports fields, music halls, and convention auditoriums). AEDs are often lifesaving devices for heart attack victims before reaching the hospital ER.
If you were experiencing chest pain, the attending physician might administer various commonly used narcotics (painkillers, such as morphine) and would give you oxygen, usually a part of management. In addition, nitroglycerin is often used, because it temporarily opens up narrowed arteries, improving blood flow to your heart muscle.
When the emergency treatment is completed in the ER, those in attendance would transfer you to the coronary (cardiac) care unit (CCU) for further management along with more diagnostic tests.
After they fully evaluated you in the CCU, they would attempt coronary angioplasty (dilatation of narrowed or blocked coronary arteries) after a coronary angiogram.
If you did not respond satisfactorily to coronary angioplasty (another term for percutaneous transluminal coronary angioplasty, or PCTA) or those attending you found it to be technically difficult, they would consider a coronary artery bypass graft (CABG).
Terms:
Cardiopulmonary resuscitation (CPR) – life-saving technique using artificial respiration and cardiac massage to restore normal functions of the heart and lungs after cardiac arrest.
Thrombolytic therapy – intravenous administration of medications that dissolve blood clots blocking the coronary arteries.
Taking aspirin while an acute heart attack is in progress can reduce the death rate by 25%.
Avoiding the truth can literally be fatal to heart attack victims.
What medications are commonly used to treat heart attack victims?
There are many medications used in the treatment of a heart attack, but the most important medications are various thrombolytic agents (medications to dissolve the blood clots in the coronary arteries). Commonly used agents are digoxin (often called heart pill), beta-blockers, angiotensin-converting enzyme (ACE) inhibitors, diuretics (often called water pills), angiotensin II receptor blockers, and spironolactone (Aldacton). The scope of this book does not permit detailed discussion of these medications.
When these medications are not effective, various medical/surgical devices, such as a heart pump (called left ventricular assist devices), a biventricular artificial cardiac pacemaker, and even an artificial heart have been used in the management of advanced CHF. In addition, the treatment of the underlying coronary artery disease such as coronary artery dilatation and coronary artery bypass surgery is very important in the management of CHF. When all of this management is not effective, the transplantation of a new heart must be considered as a last resort in the treatment of far-advanced CHF. When advanced CHF fails to improve in heart attack victims, a fatal outcome is often unavoidable.
An additional medication is found in the common aspirin. Heart attack victims are advised to chew one regular-strength aspirin when first experiencing chest discomfort. Aspirin is effective in inhibiting blood clotting in the coronary arteries. ER personnel often use “super aspirin” (a platelet II-b/III-a receptor blocker) together with a thrombolytic agent. Super aspirin has been found to be more potent than regular aspirin in preventing new blood clot formation. Anticoagulants (blood-thinning drugs), such as heparin or hirudin, often can prevent blood clotting. The relief of chest pain usually requires various narcotics (painkillers), such as morphine. Additionally, doctors commonly use nitroglycerin to relieve chest pain because this drug temporarily opens up narrowed coronary arteries and improves blood flow to the heart muscle.
Various beta-blocking medications are effective in lowering rapid heart rates and blood pressure so that the workload of the damaged heart muscle can be reduced. Anti-arrhythmic agents include various medications (e.g., lidocaine, procainamide, amiodarone) needed to manage and prevent a variety of rapid heart rhythms. Lipid or cholesterol-lowering drugs (e.g., statins, niacin) will reduce blood cholesterol. They’re beneficial if given early after a heart attack for a better chance of survival. The management of various complications requires many other medications (e.g., digoxin, antihypertensive drugs).
Term:
Anti-arrhythmic agents – medications such as quinidine or procainamide (Pronestyl) used for the prevention and treatment of various cardiac arrhythmias.
{kind=link}