What is ANGIOPLASTY and STENTING?
MAYO CLINIC – Coronary angioplasty and stents
How do I prepare for coronary angioplasty?
Unless you were already hospitalized, you would be admitted to the hospital on the day of the procedure or on the night before. You would be told not to eat or drink anything after midnight (at least 6-8 hours before the procedure). When the hospital staff were certain that you understood the procedure (its purpose, potential benefits, and possible risks), you would sign a consent form.
Before the procedure, after routine blood tests, the staff would perform an electrocardiogram (ECG) and a chest x ray. They would clean and shave your groin area (or your arm area in some cases) to prevent any infection before inserting the catheters (also as a part of the procedure). They would insert a small intravenous needle (IV line) into an arm vein for administering fluids and medications as needed. It would be a good idea to empty your bladder as completely as possible before the procedure starts. (Of course, a bedpan or urinal would be available during the procedure).
What is a coronary stent, and when is it used?
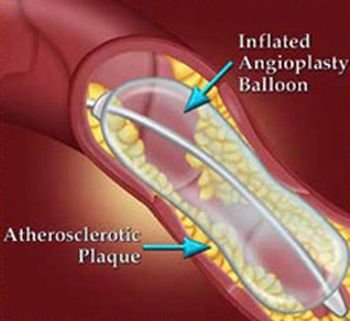
A coronary stent is a relatively new device implanted permanently in the diseased coronary artery to keep the diseased coronary artery open during and after coronary angioplasty. It is used in up to 60 to 80% of patients who undergo PTCA. The stent is a fine slotted, metallic coil, tube, or mesh structure inserted into the diseased coronary artery at the site where PTCA procedure dilated the blocked or narrowed coronary artery. The stent can reduce various complications, such as a new heart attack or a restenosis of the coronary artery. Research has shown that the restenosis rate after a simple coronary angioplasty without a stent is 30 to 40%, but the restenosis rate is reduced to 20% when a stent is used. Thus, the stent is used practically for every patient who undergoes coronary angioplasty.
The coronary stent is mounted on a balloon catheter and delivered to the site of severe narrowing or blockage of the coronary artery. When the balloon is inflated, the stent expands and is pressed against the inner wall of the diseased coronary artery. After the balloon is deflated and removed, the coronary stent permanently remains in place to prevent restenosis.
Several different kinds of stents are produced in various designs, but the most commonly used stent is the Palmaz-Shatz stent. This stent is a small, slotted, stainless-steel tube about half an inch long, and it weighs as little as a straight pin. It is as narrow as a piece of thin noodle. One or more coronary stents may be used in the coronary artery when the narrowed or blocked segment of the artery is long. New tissue will slowly grow over the stent within a few weeks and will completely cover the stent.
What medications are commonly used during and after coronary angioplasty?
Restenosis of the coronary artery during or shortly after a successful coronary angioplasty is often (but not always) due to blood clots. Doctors frequently use anticlotting agents (medications to prevent blood clots), such as aspirin, heparin, coumarin, or combinations of these drugs, during and after the coronary angioplasty to prevent restenosis. Actually, aspirin is found to be more effective than heparin for this purpose.
New anticlotting agents, such as tirofiban or clopidogrel, may be effective in preventing restenosis when they are administered in combination with heparin or aspirin. However, in some cases, restenosis of the diseased coronary artery cannot be prevented by using the above-mentioned anticlotting drugs during or after angioplasty. That’s because restenosis in some cases is due to unknown causes.
What are the potential risks involved with coronary angioplasty?
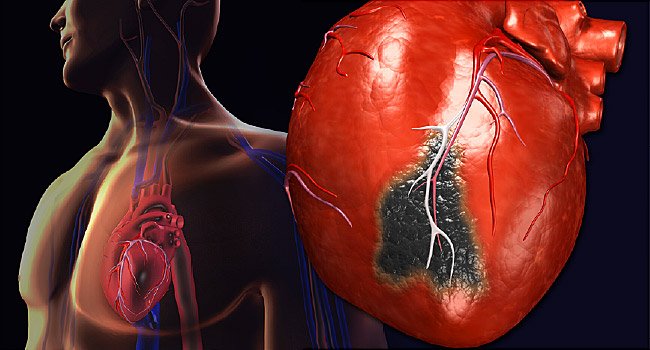
The risks from coronary angioplasty are generally minimal, and its significant benefits usually outweigh the risks in treating heart attack patients. Potential risks involved with coronary angioplasty may include tearing or cracking of the coronary artery lining, which might close the treated artery, or cause a new heart attack or stroke or even (rarely) death. Because of such risks from coronary angioplasty, a cardiac surgical team must stand by during an angioplasty.
{kind=link}