Treatment decision-making
Having carried out a biopsy and appropriate imaging, a decision has to be made about the treatment approach for the patient. An important initial decision is whether or not cure is feasible. If treatment is going to be essentially palliative, this must be factored into decision-making – quality of life becomes paramount. If treatment is potentially curative, then different considerations apply – research has shown that patients will endure considerable side effects in return for a chance of cure. Whether the aim is cure, life prolongation, or palliation of symptoms, a range of approaches are available and may be used either alone or in combination. Decisions need to be reviewed on a regular basis and treatment adapted in accordance with side effects and tumour response – that is, whether or not things are improving.
Increasingly, in major healthcare systems, these decisions are not made by individual doctors but by a multi-disciplinary team, usually abbreviated to MDT (in the UK, this is now mandatory if the hospital is to receive reimbursement for cancer therapy). Typically, these teams will comprise surgeons, radiation and medical oncologists, radiologists, pathologists, and specialist nurses. The MDT will review the baseline information (termed staging information) prior to the consultation with the patient to review the various test results. Generally, these decisions will be based on national or international guidelines on best practice. The results and treatment options will then be discussed with the patient in the clinic, and the clinical plan finalized.
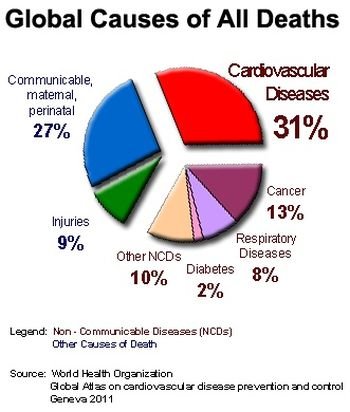
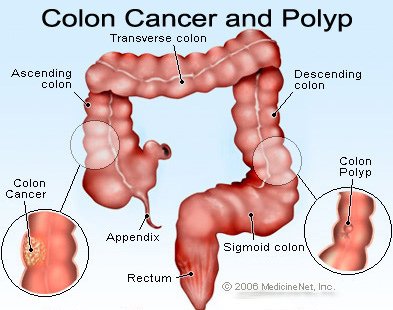
The various treatment modalities will be dealt with in turn, but before doing so, it may be helpful to give a broad breakdown of the relative importance of the treatment modalities. . For example, bladder cancer can be managed either by surgery to remove the bladder (cystectomy) or by radiotherapy to destroy the tumour, with surgery reserved for salvage of radiotherapy failures. In the USA, very few patients are managed electively with radiotherapy, which is reserved mostly for palliation (symptom control) in the elderly and frail. In contrast, in the UK, around two-thirds of patients are managed with primary radiotherapy, with surgery focused on the younger, fitter patients. These differences in practice stem largely from the differences in the UK and US health economies rather than any evidence-driven differences. The essential principle underlying the distribution is that around 30% of cases are only very locally invasive – for example, basal skin cancers (commonly called rodent ulcers) – and require a very limited local therapy, usually surgery but occasionally radiotherapy. Of the rest, around 40% of patients end up with widespread cancer and 30% have locally advanced cancer, which can be eradicated by local/regional treatments such as surgery or radiotherapy. As already indicated the precise split varies in part by geography but also varies with anatomical site. For example, cancer of the colon is best treated with surgery rather than radiotherapy, as a normal large bowel is relatively intolerant of radiotherapy, and also targeting a mobile structure is clearly problematical. On the other hand, cancer of the uterine cervix (neck of the womb) is now predominantly treated by radiotherapy combined with simultaneous chemotherapy, with surgery reserved for salvage cases plus a limited role in assessing the disease for local spread.
Of the patients who end up with advanced cancer, around half present with this in the first place, the other half start out with apparently localized disease but then subsequently relapse with more widespread problems. Of patients who develop advanced (usually called metastatic) cancer, the majority will have essentially incurable disease. These will be diseases like advanced lung, bowel, breast, prostate, or liver cancer – the major cancer killers. A minority will have potentially chemocurable diseases such as testicular cancer, lymphoma, leukaemia, or certain childhood cancers.
It can be seen from this breakdown that the majority of patients cured of cancer in the 21st century are treated with modalities developed initially in the 19th century – surgery and radiotherapy. The major drug treatment advances, which drive so many of the news headlines, started in the mid-20th century and mostly extend lives in advanced disease rather than actually curing patients. This fact is well known to public health doctors but less well appreciated by the general public. It follows from this that in poorer economies; the maximum impact on cancer will be obtained by putting in place good basic surgery and radiotherapy. The best illustration of this is the survival rates worldwide for rectal cancer, for which the best results are obtained in Cuba, renowned for its well-organized medical care but with very limited access to the more expensive new drugs. Where resources are limited, cancer chemotherapy is best focused on the rare chemocurable cancers such as childhood leukaemia and testicular cancer. As these cancers mostly occur in younger people, the impact from drug spend in this area on life years saved is disproportionately high compared to spending on end-of-life cancer drugs in older patients. Drug therapy for advanced disease occurring in later life tends to have a much smaller impact on cure rates. Even if cures were common, the patients themselves are older and thus have more limited life expectancy anyway.
Surgery
Surgery clearly dates back millennia, but the era of cancer surgery really dates back to the development of effective anaesthesia in the mid-19th century, which moved surgery from the ghastly, last-ditch ‘gore-fest’ of emergency amputations to controlled dissections. As already discussed, surgery to remove the tumour is one of the mainstays of cancer therapy (together with radiotherapy), and despite advances in drug treatment seems set to remain so for the foreseeable future. Increasingly, surgeons are developing minimally invasive (often called keyhole) techniques to operate without performing large incisions. These have the advantage of rapid postoperative recovery, but do increase operation times and are technically challenging. These techniques do allow older, frailer patients to be operated on due to the faster recovery times. They are also more generally attractive to all patient groups as they are less painful in the recovery period and rehabilitation to full normal function is quicker. Against this, operating via long metal tubes whilst peering down a modified telescope has been likened to tying your shoelaces with chopsticks, making exponents of open surgery claim that the key cancer outcomes – completeness of tumour removal, for example – may be compromised. Assessment of this aspect of care is made by the pathologist – a key member of the cancer team. A recent development in minimal access surgery is the robot assisted procedure. In a robotic operation, the instruments are inserted manually and then fixed into the robot arms. Viewing ports are inserted and the surgeon operates at a console separate from the patient – essentially using computer games technology to manipulate the instruments remotely. There are potential downsides to this exciting technology – for example, the set-up time for the robot instruments is longer than directly manipulated ‘keyhole’ instruments. Also, the machines themselves cost around £1,000,000 to buy and approximately £150,000 per year to run. This is a considerable additional outlay over and above all the general infrastructure of operating theatres, wards, anaesthetic departments, and so on. Whether ultimately this will turn out to be both clinically and cost effective clearly remains to be seen. Certainly in the USA, there is now very strong consumer/patient demand for robotic surgery that may ultimately override the colder clinical considerations. Radiotherapy
Radiotherapy is another 19th-century technology still going strong in the 21st century. Roentgen made the key observations underpinning modern radiotherapy in 1895 when he observed that invisible rays (which he called X-rays’) were produced when electrons were fired at a target in a vacuum – revealed by their ability to blacken photographic film. It was rapidly realized that X-rays were transmitting energy and that this energy could be potentially focused for treatment as well as imaging. Within a matter of months, the first patients with skin tumours were treated – a breathtaking rate of innovation. The technologies of both imaging and therapy have gradually been refined and improved over the last century or so, and now form key components of modern cancer therapy. Indeed, as already noted, the most effective parts of modern cancer therapy remain surgery and radiotherapy, with the additional gain from drug treatment in terms of cure rates being relatively marginal. In wealthy first-world economies, drug treatments can clearly be funded over and above these two key planks of therapy. However, in poorer countries, where difficult choices have to be made, very few drugs offer good value for money in curative terms compared to surgery and radiotherapy.
After the initial observations of the effects of X-rays, either electrically generated or produced by using radioactive isotopes, the technology has been progressively refined. Initial technology based on the vacuum tubes described by Roentgen in the 19th century gave a beam which could penetrate to internal organs but which deposited considerably more of the dose nearer the skin. In the 1950s, much more powerful, so-called mega-voltage machines became available. These were based on the artificial isotope Cobalt-60, now superseded by an electrically based device called a linear accelerator, usually abbreviated to linac. These latter machines used the magnetron valve developed in the Second World War for radar. The pulsed energy can be used to ‘shove’ electrons into the target at much higher energies with much better properties for treating deep-seated tumours – a sort of electronic ploughshare from a high-tech sword.
Modern radiotherapy can be very precisely targeted by integrating treatment delivery with detailed imaging. Side effects arise in two ways. In structures such as skin, gut lining, and the mouth, the effects can be likened to sunburn, with severity depending on the dose received. Effects experienced depend on the site treated and may include diarrhoea with lower bowel treatment, or sore mouth, hair loss, and reddening in treated skin, and so on. A second group of side effects is experienced in solid structures such as lung and kidney. In these organs, there is little immediate effect, but if critical dose constraints are exceeded, the irradiated tissue will progressively fail. Dose to critical organs adjacent to the target tumour is thus a key restriction on the delivery of radiotherapy – a certain amount of toxicity will be worth accepting in order to treat the cancer, but clearly there comes a point when the damage may outweigh the benefit. Improved radiotherapy such as intensity-modulated radiotherapy (IMRT), involving very sophisticated dose distributions which appear to ‘bend’ dose around critical structures, is increasingly becoming available but increases costs and complexity of delivery. A linked development is on-board imaging in treatment machines which can be used to give image-guided radiotherapy (IGRT) where the treatment tracks movements in the tumour from day to day. The combination of IMRT and IGRT has the potential to both increase tumour control (by ensuring treatment is on target) and decrease side effects by better sparing of uninvolved tissues.
Hormone therapy
Although chemotherapy now dominates cancer drug therapy, it was a hormone-based drug therapy that was the first successful medicinal cancer treatment. Hormone therapy for cancer dates back to the 1940s following observations made by Charles Huggins, an American urologist, on patients with advanced prostate cancer.
The pioneers of hormone therapy reasoned that if the ‘parent’ tissue needed normal hormone levels, then the abnormal tumour derived from the tissue may retain this dependence. Trials of castration in advanced prostate cancer produced dramatic results, with rapid and substantial improvements in symptoms such as pain from cancer deposits in bone. Following this, administration of female hormones, which of course suppress male characteristics, was attempted, again with dramatic results. Sadly, these endocrine effects, while substantial, would last for only 1 or 2 years, the disease then recurring. Similar effects were observed in pre-menopausal women with breast cancer following removal of the ovaries. The subsequent decades have seen the development of a whole range of hormone-based medications for both prostate cancer and breast cancer in particular. One of these drugs, the oestrogen blocker tamoxifen, is probably responsible for saving more lives than any other anticancer drug. More than half a century on, new drugs targeting the hormone pathways are still appearing in the clinic.
Chemotherapy
If members of the public are asked to name the class of drugs most associated with cancer treatment, they will say chemotherapy. The term covers a wide range of different agents with diverse origins from antibiotics to plant extracts to synthetic chemicals based on DNA. All interfere with the mechanics of cell division and, as many tissues have dividing cells, this leads to the typical side effects such as nausea and vomiting (partly from damage to the gut lining, partly from a direct effect on the brain), hair loss (damage to hair follicles), and risk of infection (damage to the production of white blood cells needed to defend against infection). We are all familiar with the images of billiard ball bald patients ‘fighting’ cancer (to use the tabloid press term). Whilst this does occur with chemotherapy, the reality is more varied, with much chemotherapy given in the outpatient setting producing little nausea or hair loss. Hair loss is hard to prevent, but it is not a uniform property of all chemotherapy drugs. Nausea and vomiting are now pretty largely preventable, allowing the administration of drugs hitherto considered too toxic, even to quite elderly patients. This is important because much chemotherapy is given for palliation of symptoms, hence quality of life is of paramount importance. There is arguably little point to life prolongation if the quality of that life is poor. The first chemotherapy drugs were based on chemicals derived from mustard gas, used extensively to ghastly effect in the First World War. It was noted that soldiers exposed to these agents who survived would experience drops in their white blood cells (the cells in the blood that are responsible for defense against infection). There is, of course, a cancer of the white blood cells – usually termed leukaemia. Trials were carried out of mustard gas derivatives such as mustine in both leukaemia and a second related group of cancers called lymphoma. Patients in these trials experienced for the first time remissions of what had previously been untreatable conditions. With drugs used singly, unfortunately these remissions turned out to be temporary. However, further drugs followed, and trials established that using these drugs in combinations could lead to cures for patients with leukaemia and lymphoma. A wave of new chemotherapy drugs followed, and in the 1970s and 1980s it was widely assumed that these would in turn lead to curative therapies for most cases of advanced cancer. These drugs came from a variety of sources. Plant extracts (vincristine, docetaxel, paclitaxel), complexed heavy metals (cisplatinum, carboplatin), and antibiotics (doxorubicin, mitomycin) proved to be fruitful areas of discovery leading to large-scale laboratory screening programmes looking for promising chemicals in a whole range of plant and bacterial extracts. Another area of discovery was compounds derived from the components of DNA or other building blocks of the cell division process, the best example being 5-fluoro-uracil, which is a derivative of uracil, one of the components of RNA. The extra fluorine atom in the molecule allows 5FU to interact with DNA and RNA but not to be processed normally – a molecular ‘spanner’ in the works.
In the 1970s and 1980s, further notable successes followed; in particular advanced testicular cancer was transformed from a lethal to a highly curable condition. The magnitude of this success is best illustrated by seven-times Tour de France champion Lance Armstrong who was diagnosed with very extensive disease, including brain involvement. After successful extensive chemotherapy, he went on to win his first Tour, followed by a record-breaking six further triumphs. Similar successes have been seen in the leukaemias and a range of childhood cancers. Sadly, however, the major cancer killers have proved to be more resistant to chemotherapy, with cures elusive, although most tumour types will respond to chemotherapy to a degree. It was suggested that the problem may have been that insufficiently large doses of chemotherapy were being given. However, a round of trials in the 1990s showed that even extreme doses of combination chemotherapy together with a bone marrow transplant were unable to cure major killers such as advanced breast cancer.
This realization has led to a change of emphasis. The observation that advanced disease, while incurable, would respond to chemotherapy for a while led to the testing of chemotherapy in the setting of early disease, as had previously been done with hormone therapy. It was known that many patients with no obvious disease nonetheless later developed recurrence. This suggested that there must be very small amounts of cancer lurking undetected. The hypothesis was that giving chemotherapy early may work better than waiting for detectable relapse. Initial trials were disappointing but with hindsight were simply too small to detect the benefits. When trial results were pooled in breast cancer, it was realized that there was a benefit to early chemotherapy, with women receiving it relapsing later and surviving longer compared to those for whom chemotherapy was saved as a ‘salvage’ treatment. This is called adjuvant therapy and works on the principle that so-called ‘micro-metastatic’ disease may be eradicable; whereas once the disease is visible on a scan it is incurable. Essentially, modern scanners, whilst very sensitive, are unable to detect tumours smaller than a few millimeters across. Hence we cannot distinguish between people who have been cured by initial surgery or radiotherapy and those who have apparently normal scans but in reality harbour small residual tumour deposits destined to cause relapse in the future. Subsequent studies have refined the drug combinations used and also the groups of women deriving most benefit. The problem with adjuvant therapy is that many women will do well just with surgery and radiotherapy, and thus derive no benefit from the chemotherapy, only toxicity and potential harm. This risk is greatest for those with lowest risk of disease recurrence, either due to less aggressive disease or high risk of death from other causes (for example, the very elderly).
More recently, greater emphasis has been placed on the role of chemotherapy in palliation of symptoms. This may seem like an oxymoron – giving toxic drugs to reduce suffering. However, improved symptom control, in particular with drugs that prevent the severe nausea previously associated with chemotherapy, has transformed the value of these agents for palliation. The survival gains seen are often relatively modest – typically a matter of months – leading to researchers developing methods for measuring quality of life. This allows comparison of toxic drugs producing benefit, for example by reducing pain, with alternatives often described under the blanket term of ‘best supportive care’ – painkillers, radiotherapy, and so on.
These two trends – adjuvant and palliative use – have greatly increased the cancer drug bill in the developed world (see Chapter 5) as, although the gains are relatively small, the numbers who can benefit are enormous, and this has resulted in widespread use of chemotherapy in relatively elderly cancer patients.
Monoclonal antibodies
Antibodies are a key component of the body’s immune defences. Each antibody comprises a constant region and a variable region. The variable region is responsible for the binding of the antibody to its target. The normal function of antibodies is to bind to invading infectious organisms – viruses, bacteria, and so on. When exposed to a new infection, the body’s white blood cells identify it and select the cells (called lymphocytes) with the antibody-variable region best able to stick to and disable the invader. Production of the relevant cells is massively increased, followed by increased production of antibodies able to bind to the invader. Once bound, other immune cells identify the antibody-coated invaders and ingest them, using the antibody-constant region as a ‘hook’ for pulling them out of the circulation. The development of an immune system is one of the key evolutionary steps necessary for the existence of complex multicellular organisms. Those born with inherited defects in their immune systems struggle to survive childhood, underlining the importance of this function.
In the 1970s, technology was developed to exploit the ability of the immune system by manufacturing antibodies against ‘artificial’ targets such as cancer cells. These engineered targeted antibodies are called monoclonal antibodies – antibodies made by a single clone of cells – and can be made to stick to pretty much any chosen target. By picking targets on cancer cells, these natural molecules can be own right. When they first appeared, it was thought that monoclonal antibodies would be the ‘magic bullet’ that would eradicate advanced cancer by being custom-made to order for each tumour. The reality sadly proved to be less dramatic, but 30 years on, monoclonal antibodies are now hitting the clinics in increasing numbers.
The best-known monoclonal antibody is probably trastuzumab, more often referred to by its trade name of Herceptin. The drug targets a protein on the surface of cancer cells known as HER2, part of a family of what are called growth factor receptors. These are best thought of as on/off switches regulated by circulating proteins (in this case called heregulin). Around one-third of breast cancers have an abnormal form of HER2 on the cell surface, essentially resulting in the switch being turned permanently ‘on’. Breast tumours that are HER2-positive grow faster and more aggressively than those that are HER2-negative. Targeting HER2 on the cell surface thus seemed a logical strategy and monoclonal antibodies a good way of going about it. Initial studies were carried out in women with HER2-positive tumours and confirmed that the approach worked, with the drug being licensed in 2002. Although results were positive, with shrinkage of tumours seen, they were not as dramatic as may have been hoped for. Nonetheless, further trials were deemed worthwhile, this time using Herceptin in conjunction with chemotherapy for advanced disease. These trials produced more striking results, with women receiving Herceptin surviving around 50% longer than those receiving just chemotherapy.
The next stage of development proved to be even more interesting. Having shown benefit in incurable disease, the next step was to test the drug in patients with earlier disease at a potentially curable stage, a strategy that had already proved successful with hormone therapy and chemotherapy. The Herceptin adjuvant trials were an oncological triumph, with a halving of the relapse risk and the possibility that some of the previously incurable women were actually cured. There was a catch, however. Most women with early HER2-positive breast cancer actually already had a good outlook just with surgery, radiotherapy, and chemotherapy. If a woman is already cured by these treatments, she clearly cannot benefit from any further treatment (and may indeed be harmed, as Herceptin carries a risk of heart disease).
Conversely, some women will still die despite all current therapies, and therefore they too will benefit relatively little. In between are the real winners, converted from those destined to relapse to those potentially cured. This means that in the adjuvant (preventative) setting, the number needed who must be treated to benefit one of the real winners is high, maybe as many as 20. As the cost of Herceptin is substantial (around £30,000 per year), the effective cost per woman saved can be estimated as around 20 × 30,000 = £600,000. Unsurprisingly, therefore, when the drug was licensed for adjuvant use, a further storm of controversy followed – how much is it reasonable to spend to save one life?
Targeted molecular therapies
The DNA revolution and the sequencing of the entire human genome always promised that the benefits would result in better medicines. As more and more genes were cloned, it became possible to map the genes that were abnormal in cancer cells compared to normal cells. Once a key gene is identified, it then became possible to design drugs to target the abnormal gene or, more precisely, its associated protein product. One way to target therapies is with antibodies, as described above. The other way, now generating large numbers of new drugs, is to produce chemicals that interfere with the function, either of the abnormal protein itself or of one of the other elements of the same pathway in the cell. The first and probably best example of the first strategy is the leukaemia drug imatinib (Glivec). A form of leukaemia called chronic lymphocytic leukaemia (CLL) has long been known to be characterized by the presence of a so-called ‘Philadelphia chromosome’. This abnormal chromosome is a fusion of two different chromosomes and results in the production of an abnormal protein derived from two different genes – called the bcr-abl fusion protein. Detailed molecular biology studies established that bcr-abl was both necessary and sufficient (the key conditions for a candidate new drug development) to drive the CLL cells, making it an ideal target. The drug imatinib was the first drug to successfully hit the target and it transformed the prognosis for CLL, with prolonged remissions occurring in patients resistant to the chemotherapy drugs previously used. Sadly, however, the remissions, while lengthy, were not permanent – the cancer cells eventually became resistant. This has been a feature of the targeted small molecular therapies – they are often exquisitely effective, with low side effects compared to chemotherapy, but generally do not lead to cures. However, as already noted in the chemotherapy section with leukaemia, initial use of these drugs singly also only produced remissions but not cures, so hopefully combination use will prove similarly beneficial. Time will tell.
The second approach to targeted therapy is to aim for the pathway that is linked to the ‘core’ abnormality. The best example of this is the recent transformation of kidney cancer therapy. Until recently, advanced kidney cancer was all but untreatable, with only two drugs licensed, interferon and interleukin-2, both of very limited effectiveness. Most kidney cancers occur ‘spontaneously’, that is to say, no other family members develop the same cancer. It had been observed many years ago that rare families developed the same tumours, often at a very young age. One such inherited syndrome was described by von Hippel and Lindau and now bears their names. Patients with von Hippel Lindau (VHL) syndrome develop multiple early kidney cancers
as part of the disease. Microscopically, the VHL cancers resembled the much more common, noninherited cancers, so it was suspected that abnormalities in the VHL gene may be present in the spontaneous cancers, and this did indeed turn out to be the case. However, the problem in patients with VHL syndrome is that the normal function in the VHL protein is missing; hence targeting the VHL protein itself would only make the problem worse. Study of the VHL pathway revealed that as a result of VHL under activity, proteins normally suppressed by the VHL protein became overactive. These include proteins driving the cells to divide and a further family of molecules driving the production of new blood vessels. Drugs were developed which targeted members of this pathway, either up- or downstream of the misfiring VHL protein, including three small molecular therapies, sunitinib, sorafenib, and temsirolimus, and a monoclonal antibody called bevacizumab.
Trials of these drugs have resulted in the treatment of advanced kidney cancer being revolutionized, with all four drugs licensed since 2006 and a further raft of additional drugs also heading into the clinic. As with CLL, however, although for the first time large advanced tumours could be made to shrink, the drugs do not result in cures in most cases, and treatment resistance develops with time. Trials are now focusing on adjuvant therapy, sequencing, and combinations in the hope that further survival gains can be made.
As with the Herceptin story above, the drugs have caused huge controversy due to their cost – patients need to be treated continuously rather than with a limited course of treatment, as was previously the norm with treatments such as chemotherapy. The drugs are expensive – around £25,000–£30,000 per year of treatment – with consequent variations in access. Unlike with Herceptin and breast cancer, however, purchasing authorities in a range of countries, including Canada, Australia, Scotland, and England, have been more resistant to funding treatments for a group of predominantly elderly male patients than they were for the very vocal women’s breast cancer lobby.



{kind=link}