Diabetes, Long Term Complications
Living with Diabetes – Complications
Long-term complications
Before insulin was discovered, people with diabetes did not survive long enough to develop diabetic complications as we know them today. In the early days after the great discovery, it was widely believed that insulin cured diabetes. We are now in a better position to realize that, although insulin produced nothing short of miraculous recovery in those on the verge of death and returned them to a full and active life, it is no cure for the condition. However, used properly, insulin results in full health and activity and a long life.
Life expectancy has increased progressively since insulin was first used in 1922 and there are now many thousands of people who have successfully completed more than 50 years of insulin treatment. Increased longevity has brought with it a number of the so-called ‘long-term complications’, some of which (such as heart disease and gangrene of the legs) occur not uncommonly in people who do not have diabetes and are generally considered to be inevitable consequences of the ageing process (we all have to die some time!). Others are not seen in people without diabetes.
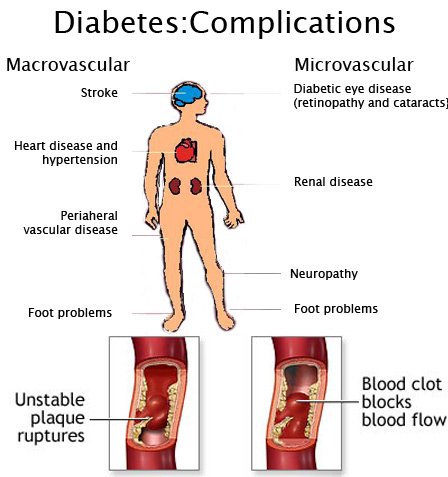
These conditions are therefore considered the long-term complications specific to diabetes: the three most important are eye damage (retinopathy), nerve damage (neuropathy) and kidney damage (nephropathy). Diabetic retinopathy can lead to loss of vision and indeed is the commonest cause of blindness registration in people under 65 in the UK. Fortunately it leads to visual loss only in a small proportion of people. Diabetic neuropathy, by leading to loss of feeling, particularly in the feet, makes affected people susceptible to infections and occasionally gangrene, leading to the risk of amputation. It can also cause impotence. Diabetic nephropathy can cause kidney failure and is now the commonest reason for referral for renal dialysis and transplantation in the UK and Europe in young people, although again it occurs only in very small numbers.
It is not surprising that people dread the thought of diabetic complications. In the past they worried but did not ask about them as they were a taboo subject. They were only for discussion between doctors and not between doctor and patient. The world has changed and today people rightly demand to know more about their condition (‘Whose life is it anyway?’) and the majority now find out about the dreaded ‘complications’ soon after they are diagnosed. There are so many old wives’ tales circulating about diabetic complications and it is perhaps the most important area in diabetic counselling where the facts rather than opinions must be stated.
Although medical science has made impressive progress since the discovery of insulin, there is still a long way to go. The scientific evidence from studies of experimental diabetes in animals is strongly in favour of the specific complications of diabetes being directly related to the degree to which the blood glucose is raised. Conversely their prevention is possible by tight control of the blood glucose concentration. We believe that the specific diabetic complications in humans are also a direct result of a raised blood glucose level over many years and that they are all preventable by keeping blood glucose values and HbA1c values normal. This view has been supported by the results of a very large multicentre clinical trial in the USA – the Diabetes Control and Complications Trial (DCCT), and the UK Prospective Diabetes Study (UKPDS) in the UK, which conclusively proved that complications can be avoided by strict blood glucose control.
Some of the questions in this chapter relating to eyes and feet are not strictly questions about complications, but as they do not easily fit in anywhere else in the book they have been included in this chapter under their specific headings.
General questions
Can someone who is controlled only by diet suffer from diabetic complications?
Complications may occur with any type of diabetes. The cause of diabetic complications is not completely understood, although bad control of diabetes is the most important predisposing factor. The duration of diabetes (the length of time for which you have had it, diagnosed or not) is also important – complications are rare in the first few years and occur more commonly after many years.
People treated with diet alone are usually diagnosed in middle or later life. At the time of diagnosis, the disease may have been present for a long time, often many years, without the person being aware of it, and therefore without any attempt being made to control it. Thus it is not surprising that complications can occur in some people even when they are treated with diet alone. Good control in these people is clearly just as important as in people who have treatment with tablets or who have Type 1 diabetes.
My child has had diabetes for 3 years and I am trying to find out more about the disease. I recently read a book, which said that some people with diabetes may go blind. I don’t know if this is true and find it very upsetting. Surely they shouldn’t be allowed to write such things in books that young people might read?
You raise a very important matter. Diabetes was almost always fatal within 1 or 2 years of diagnosis until the outlook was revolutionized by the discovery of insulin. None the less, it still required a lot of work and experimental development in the manufacture of insulin before someone with diabetes was able to lead an almost normal life, with the aid of insulin injections, as they do today.
After several years it became obvious to doctors that some people were developing what we now call ‘chronic complications’ or ‘long-term complications’. It was clear that these took many years to develop. This became the object of a massive research drive, requiring the investment of much effort and many years of work by doctors and other scientists. We now understand how some of these complications occur, and we know how to treat them if they occur. We realize that strict control of diabetes is important in their prevention. For this reason, all doctors and other medical personnel treating people with diabetes spend much of their time and effort trying to help them improve their control and keep their blood glucose as near normal as possible. These complications do not occur in all people by any means, although nowadays, with people living longer than ever before, the complications are becoming more important.
You ask whether facts like these should be made available to people with diabetes. The majority of people like to be correctly informed about their condition, its management and its complications. Modern treatment involves increasing frankness between doctors and patients in discussing all aspects of the condition. A survey among our own patients with diabetes showed the majority expected to be told the facts about complications.
What are the complications and what should I keep a lookout for to ensure that they are picked up as soon as possible?
The complications specific to diabetes are known as diabetic retinopathy, neuropathy and nephropathy. Retinopathy means damage to the retina at the back of the eye. Neuropathy means damage to the nerves. This can affect nerves supplying any part of the body but is generally referred to as either ‘peripheral’ when affecting nerves supplying muscles and skin, or as ‘autonomic’ when affecting nerves supplying organs such as the bladder, the bowel and the heart. Nephropathy is damage affecting the kidney, which in the first instance makes them leakier, so that albumin appears in the urine. At a later stage it may affect the function of the kidneys and in severe cases lead to kidney failure.
The best way of detecting complications early is to visit your doctor or clinic for regular review. Regular attendance at the diabetes clinic is important so that complications can be picked up at an early stage and if necessary treated.
Prevention is, however, clearly better than treatment and, if you can control your diabetes properly, you will be less likely to suffer these complications.
I am very worried that I might develop complications after some years of having diabetes. Is it possible to avoid complications in later life? If so, how?
Yes. We believe that all people could avoid complications if they were able to control their diabetes perfectly from the day that they were diagnosed. There are now many people on record who have gone 50 years or more with Type 1 diabetes and are completely free from any signs of complications. The best advice we can give you on how to avoid complications is to take the control of your blood glucose and diabetes seriously from the outset and to attend regularly for review and supervision by somebody experienced in the management of people with diabetes. Focus on learning how to look after yourself in such a way that you can achieve and maintain a normal HbA1c level. If you can do that and keep your HbA1c normal, you can look forward to a life free from the risk of diabetic complications.
To what extent are the complications of diabetes genetically determined?
This is a very difficult question. Most specialists believe that there is a hereditary factor, which predisposes some people to develop complications and makes others relatively immune from them, but so far scientific proof of this is not very strong.
What is the expected lifespan of someone with Type 1 diabetes and why?
The lifespan depends to a very great extent on how old the person is when the diagnosis is made. The older the person at the time of diagnosis the closer their expected lifespan is to that of someone who does not have diabetes. Looking back to the past we know that, when diabetes was diagnosed in early childhood, the lifespan of people with Type 1 diabetes was generally reduced, mainly because of premature deaths from heart attacks and kidney failure. We know, however, that the lifespan has improved with better medical care. We believe that the life expectancy of a child diagnosed with diabetes in the 1990s is longer than ever previously possible and may be nearly as good as an equivalent child who does not have diabetes. We also know that longevity is greatest in people who make regular visits to their clinic and who keep their diabetes under strict control. Those who die prematurely are more likely to be those who do not attend clinic regularly, are not being supervised adequately and do not control themselves well, and who smoke.
My diabetes specialist has said that it does not follow that badly controlled people get all the side effects and ill health in later life; often the reverse is true. Is this really so?
There is an element of truth in this but the word ‘often’ should be replaced by ‘very occasionally’. Well controlled people rarely become ill and develop side effects, whereas people who have unstable and unbalanced diabetes often develop ill health and side effects in later life. This has been confirmed by the results of the Diabetes Control and Complications Trial (DCCT) in the USA, and the UK Prospective Study (UKPDS) in the UK.
For the last two years my cheeks have become increasingly hollow although my weight is static – is this due to diabetes?
Quite a lot of middle-aged and elderly people become slim up top and pear shaped below, whether or not they have diabetes. However, there is a rare form of diabetes called lipoatrophic diabetes and this could possibly be the explanation for the hollowing of your cheeks. This is not a recognized complication of diabetes but a rare form of the condition. Mention it to your doctor the next time you go to your diabetes clinic.
I have had diabetes for the past 10 years and have recently developed an unsightly skin condition on my shins. I was referred to a skin specialist who told me that it was related to my diabetes and would be very difficult to cure. What is it and why does it occur?
Necrobiosis lipoidica diabeticorum (otherwise known as necrobiosis) is a strange non-infective but unsightly condition that most commonly appears on the shins, although it may occasionally appear elsewhere. It may occur in people years before they develop diabetes or at any time thereafter. Nobody knows much about it and treatment can be very disappointing, but achieving good control of diabetes may help. Local steroid injections and freezing with liquid nitrogen (cryotherapy) have been tried without much success. With time the red raised patches quieten down and usually leave transparent scars. Diabetes UK have a necrobiosis network; this enables people with the condition to get in touch with others. You can contact the Diabetes UK Careline for more information.


{kind=link}