VIDEO
Fault Lines : Fast food, Fat profits: Obesity in America
Health Risks of Overweight and Obesity
Morbidity
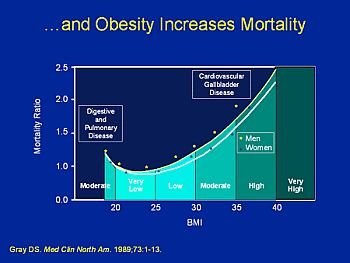
Above a BMI of 20 kg/m2, morbidity for a number of health conditions increases as BMI increases.
Higher morbidity in association with overweight and obesity has been observed for hypertension, type 2 diabetes, coronary heart disease (CHD), stroke, gallbladder disease, osteoarthritis, sleep apnea and respiratory problems and some types of cancer (endometrial, breast, prostate, and colon). Obesity is also associated with complications of pregnancy, menstrual irregularities, hirsutism, stress incontinence, and psychological disorders (depression).
The nature of obesity-related health risks is similar in all populations, although the specific level of risk associated with a given level of overweight or obesity may vary with race/ethnicity, and also with age, gender, and societal conditions.
For example, the absolute risk of morbidity in chronic conditions such as CHD is highest n the aged population, while the relative risk of having CHD in obese versus no obese individuals is highest in the middle adult years.
A high prevalence of diabetes mellitus in association with obesity is observed consistently across races/ethnicities, while the relative prevalence of hypertension and CHD in obese versus no obese populations varies between groups.
The health risks of overweight and obesity are briefly described below:
- Hypertension
Data from NHANES III show that the age adjusted prevalence of high blood pressure increases progressively with higher levels of BMI in men and women. 2 High blood pressure is defined as mean systolic blood pressure >140 mm Hg, or mean diastolic blood pressure > 90 mm Hg, or currently taking antihypertensive medication. The prevalence of high blood pressure in adults with BMI >30 is 38.4 percent for men and 32.2 percent for women, respectively, compared with 18.2 percent for men and 16.5 percent for women with BMI < 25, a relative risk of 2.1 and 1.9 for men and women, respectively.
The direct and independent association between blood pressure and BMI or weight has been shown in numerous cross-sectional studies 3-5, including the large international study of salt (INTERSALT) carried out in more than 10,000 men and women. INTERSALT reported that a 10 kg (22 lb) higher body weight is associated with 3.0 mm Hg higher systolic and 2.3 mm Hg higher diastolic blood pressure. These differences in blood pressure translate into an estimated 12 percent increased risk for CHD and 24 percent increased risk for stroke. Positive associations have also been shown in prospective studies.
Obesity and hypertension are co-morbid risk factors for the development of cardiovascular disease. The pathophysiology underlying the development of hypertension associated with obesity includes sodium retention and associated increases in vascular resistance, blood volume, and cardiac output.
These cardiovascular abnormalities associated with obesity are believed to be related to a combination of increased sodium retention, increased sympathetic nervous system activity, alterations of the renin-angiotensin system and insulin resistance. The precise mechanism whereby weight loss results in a decrease in blood pressure is unknown.
However, it is known that weight loss is associated with a reduction in vascular resistance, total blood volume and cardiac output, an improvement in insulin resistance, a reduction in sympathetic nervous system activity, and suppression of the activity of the renin angiotensin aldosterone system.

{kind=link}