VIDEO
High Blood Pressure Diet & Nutrition
(Doctor only)
Lifestyle Modification
Lifestyle modification may reduce the risk factors.
Stop smoking. This is one of the most important things patients can do, to prevent not only ischemic stroke but also heart disease, lung cancer, and head and neck cancer, etc.
Better diet. Refer patients to a dietician who can talk with patients about a low-fat diet and diabetic diet if applicable.
More exercise. Counsel the patient to adopt a less sedentary lifestyle and participate in even moderate exercise.
Blood Pressure Control
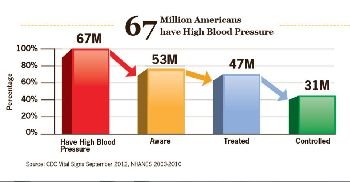
Hypertension is the single most important modifiable risk factor. JNC 7 reports that the risk of cardiovascular disease, beginning at 115/75mmHg, doubles with each increment of 20/10mmHg.
Multiple large randomized controlled trials have shown efficacy of antihypertensive treatment in primary and secondary prevention of stroke. The selection of antihypertensive remains unsettled and controversial.
Many drugs have been shown to reduce stroke in primary prevention (beta-blocker in SHEP, diuretic in SHEP and ALLHAT, calcium channel blocker in ALLHAT, ACE inhibitor in HOPE and PROGRESS, ARB in LIFE).
A combination of perindopril (Aceon), a tissue-specific ACE inhibitor, and indapamide (Lozol), a diuretic, have been shown to reduce stroke in secondary prevention even among non-hypertensive patients (PROGRESS).30 Whether this effect is due to the tissue-specific ACE inhibition rather than an ACE inhibitor class effect, or whether an ACE inhibitor needs to be used in combination with a diuretic, remains controversial.
Probably the most important point is blood pressure reduction, not the specific drug. For primary prevention, a diuretic seems to be effective and cheap. Recent meta-analysis seems to support the superiority of diuretics. JNC 7 also recommends thiazide diuretics as a first-line pharmacologic therapy, though it recognizes that more than one drug is commonly needed.
In the hospital setting, especially after a stroke, a patient’s fluid intake may be poor. A diuretic while on IV fluids does not make sense. Start a diuretic in stroke inpatients only if the patient is drinking fluids consistently
Bring down BP slowly with oral antihypertensive after acute ischemic stroke.
According to recent guidelines, the target blood pressures are the following:
<140/90mmHg
<130/80mmHg for patients with diabetes or chronic kidney disease
Remember, there is a continuous increase in risk of stroke with increase in blood pressure. There is no biological cutoff point.

{kind=link}