Although classically stroke symptoms are maximal at onset and patients gradually recover over days, weeks, and months, patients can deteriorate. People have termed the phenomenon stroke progression, stroke in evolution, stroke deterioration, and symptom fluctuation. There is no consistent terminology.
The phenomenon occurs from different causes and is incompletely understood. This chapter will discuss evaluation of potential causes, and approaches for treatment of each cause.
Probable causes
(1) Stroke enlargement (e.g., arterial stenosis or occlusion with worsening perfusion).
(2) Drop in perfusion pressure.
(3) Recurrent stroke (not common).
(4) Cerebral edema and mass effect.
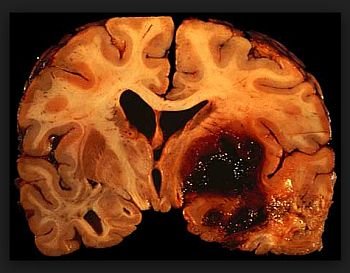
(5) Hemorrhagic transformation.
(6) Metabolic disturbance (decreased O2 saturation, decreased cardiac output, increased glucose, decreased sodium, fever, sedative drugs, etc.).
(7) Seizure, post-ictal.
(8) Symptom fluctuation without good cause (due to inflammation?).
(9) The patient is not feeling like cooperating (sleepy, drugs).
Initial evaluation of patients with neurologic deterioration
. Check airway–breathing–circulation, vital signs, laboratory tests. Is the patient hypotensive or hypoxic?
. Talk to and examine the patient. If the patient is sleepy, is it because it’s 3 a.m. or because of mass effect? Is there a pattern of symptoms (global worsening vs. focal worsening)?
. Get an immediate non-contrast head CT (to evaluate for hemorrhage, new stroke, swelling, etc.).
. Review medications (antihypertensives, sedatives).
. Observe patient, and ask nurse, for subtle signs of seizure.
. Consider MRI for arterial imaging, new stroke, stroke enlargement, swelling; TCD or CT angiography for arterial imaging; EEG to diagnose subclinical seizures.
Stroke enlargement
This occurs when there is arterial stenosis or occlusion and the hemodynamics change for whatever reason. There are no data to support that anticoagulation prevents the hemodynamic worsening, though many clinicians jump to anticoagulation with heparin. Instead, probably the best treatment is to treat the underlying stenosis/occlusion early.
The approach should be to prevent rather than treat after deterioration. The key is early imaging to detect large artery stenosis/occlusion by TCD, CT angiography, or MRI (i.e., find the high-risk patients early). Patients with minor deficits butabnormal TCD or MRA are at highest risk of progression.
Perfusion imaging may indicate areas of tissue at risk. Even without a perfusion study by MRI or CT, the finding of a small diffusion-weighted lesion on MRI and a relatively minor neurological deficit in the presence of large artery occlusion by arterial imaging indicates a high risk for progression.
In such patients, you might want to consider early intervention, such as IV thrombolysis despite low NIHSS score, intra-arterial therapy, carotid endarterectomy, or carotid stenting.
Drop in perfusion pressure
Since auto regulation is lost in ischemic brain, any reduction in blood pressure will reduce flow to penumbral regions, thereby potentially worsening the clinical deficit. This is true in both cortical and subcortical strokes. The latter have particularly poor collateral flow and may be at greatest risk for hypoperfusion-related deterioration. As a rule of thumb, mean arterial pressure (MAP) should be kept at pre-stroke levels (as a general guideline, at least 130mm Hg in hypertensive patients, and 110 in normotensive patients) in the first 24 hours, and if MAP drops below this level, and the patient deteriorates, the MAP should be increased by a fluid bolus and possibly a pressor. Don’t forget head positioning. Simply laying the patient flat, or no higher than 158 head elevation, may augment cerebral perfusion.
Recurrent stroke
Unfortunately some patients go on to have recurrent stroke.
Among atrial fibrillation patients, the stroke recurrence risk has been reported to be 5–8% in the first two weeks. There are no data to show that immediate or ‘‘early’’ anticoagulation helps, even in the setting of atrial fibrillation, because anticoagulation can lead to hemorrhagic complications.
Yet we might be underestimating the magnitude of frequency of stroke recurrence if we rely on clinical deterioration alone. One study reported stroke recurrence was detected by MRI in 34% of patients in the first week, whereas clinically only 2% stroke recurrence was noted.22 Furthermore, some patients may be at higher risk of re-embolization, especially those with associated mitral stenosis or left atrial thrombus.
Therefore, our recommendation in atrial fibrillation patients is to anticoagulate once we determine by repeat brain imaging that the infarct is small or, if large, that any acute hemorrhagic transformation or vasogenic edema is resolving. This usually means waiting 48–96 hours after the acute stroke.
In a larger population-based study, large artery atherosclerosis was associated with highest risk of stroke recurrence. This supports the recommendation to perform carotid revascularization (endarterectomy or stenting) earlier than later.